Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Being Respected by Nurses: Measuring Older Patients' PerceptionsDocument12 pagesBeing Respected by Nurses: Measuring Older Patients' PerceptionsAurora Violeta Zapata RuedaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Applied Nursing Research: Contents Lists Available atDocument10 pagesApplied Nursing Research: Contents Lists Available atAurora Violeta Zapata RuedaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Angustia CovidDocument3 pagesAngustia CovidAurora Violeta Zapata RuedaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Zma001307 PDFDocument8 pagesZma001307 PDFAurora Violeta Zapata RuedaPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Community Perception Regarding Childhood Vaccinations and Its Implications For Effectiveness: A Qualitative Study in Rural Burkina FasoDocument10 pagesCommunity Perception Regarding Childhood Vaccinations and Its Implications For Effectiveness: A Qualitative Study in Rural Burkina FasoAurora Violeta Zapata RuedaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- TERRA at Last in ANSDocument11 pagesTERRA at Last in ANSAurora Violeta Zapata RuedaPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- s12889 018 6338 0Document12 pagess12889 018 6338 0Anne Camille JonasPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Thesis Marianne VelandiaDocument103 pagesThesis Marianne VelandiaAurora Violeta Zapata RuedaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Experiencia de MuerteDocument11 pagesExperiencia de MuerteAurora Violeta Zapata RuedaPas encore d'évaluation
- Copia de PeruEnglish Aug2011copyrightjeanwatsonDocument52 pagesCopia de PeruEnglish Aug2011copyrightjeanwatsonAurora Violeta Zapata RuedaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Experiences of Healthcare Professionals In.3Document6 pagesExperiences of Healthcare Professionals In.3Aurora Violeta Zapata RuedaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- SuicidioDocument29 pagesSuicidioAurora Violeta Zapata RuedaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Thompson LBW EHP 2011Document6 pagesThompson LBW EHP 2011Aurora Violeta Zapata RuedaPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Sex Difference in New BornDocument9 pagesSex Difference in New BornAurora Violeta Zapata RuedaPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Sex Difference in New BornDocument9 pagesSex Difference in New BornAurora Violeta Zapata RuedaPas encore d'évaluation
- Sex Difference in New BornDocument9 pagesSex Difference in New BornAurora Violeta Zapata RuedaPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Use of Non Pharmacological Interventions For.7Document14 pagesThe Use of Non Pharmacological Interventions For.7Aurora Violeta Zapata RuedaPas encore d'évaluation
- eNERGEY DRINKSDocument6 pageseNERGEY DRINKSAurora Violeta Zapata RuedaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- PathwayDocument8 pagesPathwayAurora Violeta Zapata RuedaPas encore d'évaluation
- Current Recommendations For Reform in Education For Health ProfessionalsDocument76 pagesCurrent Recommendations For Reform in Education For Health ProfessionalsAurora Violeta Zapata RuedaPas encore d'évaluation
- Noise in The ICUDocument7 pagesNoise in The ICUAurora Violeta Zapata RuedaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Zola1966 DolorDocument17 pagesZola1966 DolorAurora Violeta Zapata RuedaPas encore d'évaluation
- Alarmas para UCI InvestigaciónDocument7 pagesAlarmas para UCI InvestigaciónAurora Violeta Zapata RuedaPas encore d'évaluation
- Stress and Coping in Families of Patients in An Intensive Care UnitDocument1 pageStress and Coping in Families of Patients in An Intensive Care UnitAurora Violeta Zapata RuedaPas encore d'évaluation
- Aci14 Man Eye Care 2-3Document50 pagesAci14 Man Eye Care 2-3Aurora Violeta Zapata RuedaPas encore d'évaluation
- TOUS Presentation Peru AbstractDocument1 pageTOUS Presentation Peru AbstractAurora Violeta Zapata RuedaPas encore d'évaluation
- Using Qualitative ResearchDocument6 pagesUsing Qualitative ResearchAurora Violeta Zapata RuedaPas encore d'évaluation
- Short - and Long-Term Impact of Critical Illness On Relatives YaDocument18 pagesShort - and Long-Term Impact of Critical Illness On Relatives YaAurora Violeta Zapata RuedaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Post-Traumatic Stress Disorder-Related Symptoms in Relatives of Patients Following Intensive CareDocument6 pagesPost-Traumatic Stress Disorder-Related Symptoms in Relatives of Patients Following Intensive CareAurora Violeta Zapata RuedaPas encore d'évaluation
- Ocular Disease in Critical IllDocument5 pagesOcular Disease in Critical IllAurora Violeta Zapata RuedaPas encore d'évaluation
- DAR Vol1-2013Document744 pagesDAR Vol1-2013chitransh2002Pas encore d'évaluation
- Silverio Nuanez Verified ComplaintDocument10 pagesSilverio Nuanez Verified ComplaintMichael_Lee_RobertsPas encore d'évaluation
- NCAA Safety Bulletin 23-4 - AprilDocument21 pagesNCAA Safety Bulletin 23-4 - AprilAPas encore d'évaluation
- Application For Type Aircraft Training: Farsco Training Center IR.147.12Document1 pageApplication For Type Aircraft Training: Farsco Training Center IR.147.12benyamin karimiPas encore d'évaluation
- Urban Jungle 8Document3 pagesUrban Jungle 8Angel Medez GonzalezPas encore d'évaluation
- A Comprehensive Review On Evaluation of Environmental Friendly Machinability, Cutting Fluids and Techniques in Metal Cutting OperationDocument13 pagesA Comprehensive Review On Evaluation of Environmental Friendly Machinability, Cutting Fluids and Techniques in Metal Cutting OperationIJAR JOURNALPas encore d'évaluation
- Nil Queries Sheet: S. No. ProcessDocument24 pagesNil Queries Sheet: S. No. ProcessTarun BhardwajPas encore d'évaluation
- Assignment 2Document4 pagesAssignment 2LaDonna WhitePas encore d'évaluation
- WT Notes by Mohammed Ahmed PDFDocument11 pagesWT Notes by Mohammed Ahmed PDFElavarasan MathiPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
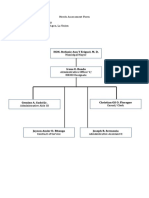
- Needs Assessment Form Company Name: HRMO Address: Sta. Barbara Agoo, La UnionDocument2 pagesNeeds Assessment Form Company Name: HRMO Address: Sta. Barbara Agoo, La UnionAlvin LaroyaPas encore d'évaluation
- 110Q Pump Catalog SheetDocument2 pages110Q Pump Catalog SheetJohnPas encore d'évaluation
- Ticket - Abibus PDFDocument1 pageTicket - Abibus PDFJosephPas encore d'évaluation
- Dissertation Sample CommerceDocument4 pagesDissertation Sample CommerceBuyPapersOnlineForCollegeCanada100% (1)
- Space Vector Modulation - An Introduction - TutoriDocument11 pagesSpace Vector Modulation - An Introduction - TutorileonardoPas encore d'évaluation
- Solution For Databases Reference Architecture For Oracle Rac Database 12c With Gad Using HdidDocument48 pagesSolution For Databases Reference Architecture For Oracle Rac Database 12c With Gad Using HdidClaudio Osvaldo Vargas FarfanPas encore d'évaluation
- Profitability Analysis (Sapphire Fibres Limited)Document5 pagesProfitability Analysis (Sapphire Fibres Limited)Aqsa MoizPas encore d'évaluation
- IPC Policy 4 PDFDocument128 pagesIPC Policy 4 PDFgary ann jimenez100% (1)
- 010 Informed Search 2 - A StarDocument20 pages010 Informed Search 2 - A StarRashdeep SinghPas encore d'évaluation
- Tutorial Chapter 3Document9 pagesTutorial Chapter 3Sirhan HelmiPas encore d'évaluation
- The Dell Direct Model: What It Means For Customers (Users) : - ProsDocument12 pagesThe Dell Direct Model: What It Means For Customers (Users) : - ProsAbhinandan MattelaPas encore d'évaluation
- A218437 HUET PDFDocument271 pagesA218437 HUET PDFKayser_MPas encore d'évaluation
- Review Accounting NotesDocument9 pagesReview Accounting NotesJasin LujayaPas encore d'évaluation
- Quote Generator DocumentDocument47 pagesQuote Generator DocumentPrajwal KumbarPas encore d'évaluation
- Guidelines in Research Proposal WritingDocument19 pagesGuidelines in Research Proposal WritingMark RelloresPas encore d'évaluation
- Mangla Refurbishment Project Salient FeaturesDocument8 pagesMangla Refurbishment Project Salient FeaturesJAZPAKPas encore d'évaluation
- SAM3-P256 Development Board Users Manual: This Datasheet Has Been Downloaded From at ThisDocument21 pagesSAM3-P256 Development Board Users Manual: This Datasheet Has Been Downloaded From at ThissunnguyenPas encore d'évaluation
- Probate Court Jurisdiction Regarding OwnershipDocument2 pagesProbate Court Jurisdiction Regarding OwnershipBnl NinaPas encore d'évaluation
- 358 IG Fashion Pack PDFDocument4 pages358 IG Fashion Pack PDFbovsichPas encore d'évaluation
- DO 31 s2020Document18 pagesDO 31 s2020charles barkleyPas encore d'évaluation
- Yosys+Nextpnr: An Open Source Framework From Verilog To Bitstream For Commercial FpgasDocument4 pagesYosys+Nextpnr: An Open Source Framework From Verilog To Bitstream For Commercial FpgasFutsal AlcoletgePas encore d'évaluation
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Gut: the new and revised Sunday Times bestsellerD'EverandGut: the new and revised Sunday Times bestsellerÉvaluation : 4 sur 5 étoiles4/5 (393)