Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Exploring Alcohol WithdrawalDocument8 pagesExploring Alcohol Withdrawalgura1999Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Functional Symptoms and Signs in Neurology: Assessment and DiagnosisDocument12 pagesFunctional Symptoms and Signs in Neurology: Assessment and Diagnosisgura1999Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Lymphomatous MeningitisDocument2 pagesLymphomatous Meningitisgura1999Pas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- SyllabusDocument76 pagesSyllabusM Usman KhanPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Carcinomatous Meningitis It Does Not Have To Be A Death SentenceDocument10 pagesCarcinomatous Meningitis It Does Not Have To Be A Death Sentencegura1999Pas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Postgraduation Employment For PharmacistsDocument10 pagesPostgraduation Employment For Pharmacistsgura1999Pas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- PEBC Sample QuestionsDocument19 pagesPEBC Sample Questionsgura1999Pas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- SPSS Workshop: Utilizing and Implementing SPSS in Our OC-Math Statistics ClassesDocument11 pagesSPSS Workshop: Utilizing and Implementing SPSS in Our OC-Math Statistics Classesgura1999Pas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A History of European Art, Part IDocument42 pagesA History of European Art, Part Igura1999Pas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Winnipeg Wading PoolsDocument8 pagesWinnipeg Wading Poolsgura1999Pas encore d'évaluation
- Administrative Manual: Director, Professional Practice Chief of StaffDocument2 pagesAdministrative Manual: Director, Professional Practice Chief of Staffgura1999Pas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- SPSS1 Finding and Managing Data For The Social SciencesDocument55 pagesSPSS1 Finding and Managing Data For The Social Sciencesgura1999Pas encore d'évaluation
- Com Medico Legal Handbook-EDocument56 pagesCom Medico Legal Handbook-Egura1999Pas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Organ Donor Management in Canada - RecommendationsDocument18 pagesOrgan Donor Management in Canada - Recommendationsgura1999Pas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Publicly Funded Immunization Schedules For Ontario - January 2009Document4 pagesPublicly Funded Immunization Schedules For Ontario - January 2009sharmas56Pas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Table 1 Minimum Separation DistancesDocument123 pagesTable 1 Minimum Separation DistancesjhonPas encore d'évaluation
- Easergy PS100 48VDC Power SupplyDocument2 pagesEasergy PS100 48VDC Power SupplyRichard SyPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Latihan To: Nilai: 7.4 Benar: 37 Salah: 13Document17 pagesLatihan To: Nilai: 7.4 Benar: 37 Salah: 13glensPas encore d'évaluation
- Exp6.Single Phase Bridge Inverter Using PWMDocument6 pagesExp6.Single Phase Bridge Inverter Using PWMAbdullah MohammedPas encore d'évaluation
- ANS: (2.59807m/s2 Horizontal) (1.5m/s2 Vertical) (12.93725 Degree Angle That The Water Surface Makes With The Horizontal)Document5 pagesANS: (2.59807m/s2 Horizontal) (1.5m/s2 Vertical) (12.93725 Degree Angle That The Water Surface Makes With The Horizontal)Lolly UmaliPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Mathematical Modeling of Mechanical Systems and Electrical SystemsDocument49 pagesMathematical Modeling of Mechanical Systems and Electrical SystemsMary DunhamPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Sci NB Mod 2 LSN 3Document4 pagesSci NB Mod 2 LSN 3Ramses octavio Rodriguez ocanasPas encore d'évaluation
- L GH Catalog PullingDocument60 pagesL GH Catalog PullingLuis LuperdiPas encore d'évaluation
- Time Value of Money LectureDocument54 pagesTime Value of Money LectureRanin, Manilac Melissa SPas encore d'évaluation
- Adaptive Cruise ControlDocument5 pagesAdaptive Cruise ControlIJIRSTPas encore d'évaluation
- Approved Project 25 StandardsDocument5 pagesApproved Project 25 StandardsepidavriosPas encore d'évaluation
- Unnatural Selection BiologyDocument2 pagesUnnatural Selection BiologyAlexa ChaviraPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Modified Phosphate and Silica Waste in Pigment PaintDocument12 pagesModified Phosphate and Silica Waste in Pigment PaintDani M RamdhaniPas encore d'évaluation
- PEDocument12 pagesPEMae Ann Base RicafortPas encore d'évaluation
- Sw34 Religion, Secularism and The Environment by NasrDocument19 pagesSw34 Religion, Secularism and The Environment by Nasrbawah61455Pas encore d'évaluation
- Spectroscopy (L-26 To 29)Document81 pagesSpectroscopy (L-26 To 29)Vashistha GargPas encore d'évaluation
- Inform LetterDocument2 pagesInform LetterMc Suan75% (4)
- DS Ltch00601daa0 R05Document4 pagesDS Ltch00601daa0 R05rajareddy235Pas encore d'évaluation
- Relationsh Between EM and Young S ModuliDocument7 pagesRelationsh Between EM and Young S ModuliDwight AndersonPas encore d'évaluation
- Predictive Maintenance Attempts To Detect The Onset of A Degradation Mechanism With The Goal of Correcting That Degradation Prior To Signiicant Deterioration in The Component or EquipmentDocument6 pagesPredictive Maintenance Attempts To Detect The Onset of A Degradation Mechanism With The Goal of Correcting That Degradation Prior To Signiicant Deterioration in The Component or EquipmentTodd BenjaminPas encore d'évaluation
- Chapter 04 Product and ServDocument43 pagesChapter 04 Product and ServAlireza AlborziPas encore d'évaluation
- Me8072 Renewable Sources of EnergyDocument13 pagesMe8072 Renewable Sources of EnergyNallappan Rajj APas encore d'évaluation
- (Eng) Zx890lch 5a Ks En316Document13 pages(Eng) Zx890lch 5a Ks En316MC TAK LEEPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- 40 RT-flex Control-System Rev01Document68 pages40 RT-flex Control-System Rev01Mayvon Botelho100% (2)
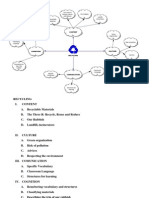
- Recycling Mind MapDocument2 pagesRecycling Mind Mapmsole124100% (1)
- Unit 2 - Presentations (Image, Impact and Making An Impression) 2Document25 pagesUnit 2 - Presentations (Image, Impact and Making An Impression) 2LK Chiarra Panaligan100% (1)
- Pre RmoDocument4 pagesPre RmoSangeeta Mishra100% (1)
- iPQ-Center Webvideo Star TTB MA R1 42 en PDFDocument32 pagesiPQ-Center Webvideo Star TTB MA R1 42 en PDFHamid KharazmiPas encore d'évaluation
- Opex and CapexDocument5 pagesOpex and CapexATM Shafiq Ul AlamPas encore d'évaluation
- John Sisler CISSP Study GuideDocument126 pagesJohn Sisler CISSP Study GuideAnthonyPas encore d'évaluation
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)