Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- T - C2019 Official Notes PDFDocument696 pagesT - C2019 Official Notes PDFPeter100% (9)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Getting Grounded On AnalyticsDocument31 pagesGetting Grounded On AnalyticsIvan Jon Ferriol100% (2)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- 2022 GKS-U University Track 2nd Round Result Successful CandidatesDocument8 pages2022 GKS-U University Track 2nd Round Result Successful Candidatesmatiasbenitez1992Pas encore d'évaluation
- Maths WorksheetsDocument6 pagesMaths WorksheetsRanoCenterPas encore d'évaluation
- Why I Let My Patients See My NotesDocument2 pagesWhy I Let My Patients See My NotesRanoCenterPas encore d'évaluation
- Color Changing Line: Date Value Before Line AfterDocument9 pagesColor Changing Line: Date Value Before Line AfterRanoCenterPas encore d'évaluation
- I Am 50+. I Face These Issues.: World Aids Day 2014Document1 pageI Am 50+. I Face These Issues.: World Aids Day 2014RanoCenterPas encore d'évaluation
- Compliance Officer: Sample Position DescriptionDocument2 pagesCompliance Officer: Sample Position DescriptionRanoCenterPas encore d'évaluation
- JAHIMA January Coding Notes RadiologyDocument3 pagesJAHIMA January Coding Notes RadiologyRanoCenterPas encore d'évaluation
- Utilization Management Director: Sample Position DescriptionDocument1 pageUtilization Management Director: Sample Position DescriptionRanoCenterPas encore d'évaluation
- CDI Week Sept 2012Document2 pagesCDI Week Sept 2012RanoCenterPas encore d'évaluation
- Toolkitforbedmanagers 100531110838 Phpapp02Document84 pagesToolkitforbedmanagers 100531110838 Phpapp02RanoCenterPas encore d'évaluation
- CDI - A Work in ProgressDocument9 pagesCDI - A Work in ProgressRanoCenterPas encore d'évaluation
- Medical Identity TheftDocument3 pagesMedical Identity TheftRanoCenterPas encore d'évaluation
- Acute Human Lethal Toxicity of Agricultural Pesticides: A Prospective Cohort StudyDocument10 pagesAcute Human Lethal Toxicity of Agricultural Pesticides: A Prospective Cohort StudyRanoCenterPas encore d'évaluation
- Appendix ADocument24 pagesAppendix ARanoCenterPas encore d'évaluation
- Solar DPR of 3 DHsDocument156 pagesSolar DPR of 3 DHsSandeep DhimanPas encore d'évaluation
- Workshop ToolsDocument2 pagesWorkshop ToolsKwee AryaPas encore d'évaluation
- HeroLab ManualDocument55 pagesHeroLab ManualColin BraddockPas encore d'évaluation
- QR Code Reader and ScannerDocument6 pagesQR Code Reader and ScannerNgwang Leonard Tenzi100% (1)
- Another Smart BookDocument22 pagesAnother Smart BookKeshav PPas encore d'évaluation
- Smart Fire Alarm System Using ArduinoDocument2 pagesSmart Fire Alarm System Using Arduinokritwik barua100% (1)
- CNC Programming & Application: Federal TVET Institute Manufacturing Technology Department Addis Abeba EthiopiaDocument58 pagesCNC Programming & Application: Federal TVET Institute Manufacturing Technology Department Addis Abeba EthiopiaGezae MebrahtuPas encore d'évaluation
- Keys For @emon9138: TRON Public Key (TRON Address)Document2 pagesKeys For @emon9138: TRON Public Key (TRON Address)Ifty ChowdhuryPas encore d'évaluation
- Strength Under Fire: Cat Fire Pump EnginesDocument4 pagesStrength Under Fire: Cat Fire Pump EnginesArgenis JimenezPas encore d'évaluation
- STS Module 3Document28 pagesSTS Module 3Arlo GutayPas encore d'évaluation
- Xirrus Enterprise WiFiDocument2 pagesXirrus Enterprise WiFiLuis MendozaPas encore d'évaluation
- Lab Exercise 1 - Getting StartedDocument8 pagesLab Exercise 1 - Getting StartedMarcos JeremyPas encore d'évaluation
- Sustaining An Ict Project For Social ChangeDocument6 pagesSustaining An Ict Project For Social Changechristianbunao1907Pas encore d'évaluation
- Zte Mg3030 ModuleDocument27 pagesZte Mg3030 Modulesardar87Pas encore d'évaluation
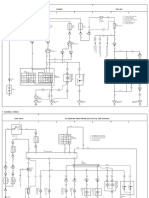
- Avanza Xenia Wiring DiagramDocument5 pagesAvanza Xenia Wiring DiagramFazri Putugerah100% (2)
- Generator Breaker Equipped With Vacuum InterruptersDocument4 pagesGenerator Breaker Equipped With Vacuum InterruptersVenna Karthik ReddyPas encore d'évaluation
- 08 - IP SubnettingDocument20 pages08 - IP Subnettingkndnew guadePas encore d'évaluation
- Presentation For Composite SlabDocument19 pagesPresentation For Composite SlabLong LothaPas encore d'évaluation
- Manual Sharp CMS-R600XDocument64 pagesManual Sharp CMS-R600Xjca16100% (1)
- Chapter 1Document6 pagesChapter 1Bhuvaneswari TSPas encore d'évaluation
- IBM Sterling Warehouse Management System: Increase Warehouse Productivity and Reduce CostsDocument5 pagesIBM Sterling Warehouse Management System: Increase Warehouse Productivity and Reduce CostsRishard MohamedPas encore d'évaluation
- Unit 2Document17 pagesUnit 2PRASATH RPas encore d'évaluation
- 19BCG1077 - Swarup DebDocument1 page19BCG1077 - Swarup DebUX ༒CONQUERERPas encore d'évaluation
- Waaree Corporate PPT - V3Document53 pagesWaaree Corporate PPT - V3Bhushan MalshePas encore d'évaluation
- Expert Office 365 Notes From The FieldDocument289 pagesExpert Office 365 Notes From The FieldYohanna Monsalvez100% (1)
- TractorsDocument12 pagesTractorsBekalu DanielPas encore d'évaluation