Vous aimerez peut-être aussi
- Acne Vulgaris Tipe Papulopustular: Bed Site TeachingDocument1 pageAcne Vulgaris Tipe Papulopustular: Bed Site TeachingSabrine DwigintPas encore d'évaluation
- Dosis Obat AnakDocument5 pagesDosis Obat AnakSabrine DwigintPas encore d'évaluation
- Anae 13101Document18 pagesAnae 13101Sabrine DwigintPas encore d'évaluation
- Hum. Reprod. Update 2012 Li 504 24Document21 pagesHum. Reprod. Update 2012 Li 504 24Sabrine DwigintPas encore d'évaluation
- Baba, 2010Document7 pagesBaba, 2010Sabrine DwigintPas encore d'évaluation
- Perbedaan Kadar Elastase Kanalis Servikalis Antara Kehamilan Dengan Ancaman Persalinan Preterm Dan Kehamilan NormalDocument6 pagesPerbedaan Kadar Elastase Kanalis Servikalis Antara Kehamilan Dengan Ancaman Persalinan Preterm Dan Kehamilan NormalSabrine DwigintPas encore d'évaluation
- Use of Anti-D Immunoglobulin in The Treatment of Threatened Miscarriage in The Accident and Emergency DepartmentDocument4 pagesUse of Anti-D Immunoglobulin in The Treatment of Threatened Miscarriage in The Accident and Emergency DepartmentSabrine DwigintPas encore d'évaluation
- Angina Caused by A Narrowing of The Blood Vessels Which Supply The Heart Muscle - Heart Attack Which Occurs When The Heart Muscle Is Deprived of Oxygen and Death of TissueresultsDocument1 pageAngina Caused by A Narrowing of The Blood Vessels Which Supply The Heart Muscle - Heart Attack Which Occurs When The Heart Muscle Is Deprived of Oxygen and Death of TissueresultsSabrine DwigintPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Complete Guide To Sexual Fulfilment Practical Handbook PDFDocument131 pagesThe Complete Guide To Sexual Fulfilment Practical Handbook PDFKathy Marsella100% (1)
- Abortion Womens Clinic in Randburg 0736613276Document2 pagesAbortion Womens Clinic in Randburg 0736613276MaamaTitiPas encore d'évaluation
- CXC Social Studies Sba 2023Document27 pagesCXC Social Studies Sba 2023David DillonPas encore d'évaluation
- Unit II Lesson I: On Responsible Parenthood and PornographyDocument22 pagesUnit II Lesson I: On Responsible Parenthood and PornographyKizea JuanicoPas encore d'évaluation
- Cock and Ball TortureDocument1 pageCock and Ball TortureDiego GomezPas encore d'évaluation
- Gynaecological History Taking - Geeky MedicsDocument7 pagesGynaecological History Taking - Geeky MedicsJahangir AlamPas encore d'évaluation
- A Rough Guide To Dirty SexDocument22 pagesA Rough Guide To Dirty Sexrakawid100% (1)
- Ior Per BrgyDocument13 pagesIor Per BrgyJuanisa Baruang BashitPas encore d'évaluation
- Daftar Pustaka Presentasi BokongDocument2 pagesDaftar Pustaka Presentasi BokongNando UspessyPas encore d'évaluation
- Aunties' For Sexual and Reproductive Health: How Unwed Young Mothers Become Advocates, Teachers and Counsellors in CameroonDocument4 pagesAunties' For Sexual and Reproductive Health: How Unwed Young Mothers Become Advocates, Teachers and Counsellors in CameroonpracticecollectionPas encore d'évaluation
- Infertility ManagementDocument56 pagesInfertility ManagementAnca RotaruPas encore d'évaluation
- Family Planning Methods Among Suarez, Iligan City FamiliesDocument13 pagesFamily Planning Methods Among Suarez, Iligan City FamiliesAngel MaePas encore d'évaluation
- GP Referral Form 2023Document1 pageGP Referral Form 2023Rahul VishwanathPas encore d'évaluation
- Answers To Your Questions About Circumcision and HIV/AIDSDocument2 pagesAnswers To Your Questions About Circumcision and HIV/AIDSAlex BrownPas encore d'évaluation
- K 2 May 12Document24 pagesK 2 May 12dreamlandbhutanPas encore d'évaluation
- Family Planning and Contrceptives For Midwifery StudentsDocument190 pagesFamily Planning and Contrceptives For Midwifery StudentsAbdusamed100% (1)
- Number of Ohio Abortion Drug Complications by AbortionistDocument2 pagesNumber of Ohio Abortion Drug Complications by AbortionistCheryl SullengerPas encore d'évaluation
- Case Study in Obstetrics and Gynaecology - Lecture Notes, Study Material and Important Questions, AnswersDocument11 pagesCase Study in Obstetrics and Gynaecology - Lecture Notes, Study Material and Important Questions, AnswersM.V. TV100% (2)
- Assignment Chapter - 4 Reproductive Health: Answers 1)Document3 pagesAssignment Chapter - 4 Reproductive Health: Answers 1)Deepanshu SinghPas encore d'évaluation
- Sentence Outline ABORTIONDocument2 pagesSentence Outline ABORTIONHano100% (1)
- Assessment of Knowledge Attitude and Practice On Emergency Contraceptive Among Goba Female High School and Preparatory StudentsDocument9 pagesAssessment of Knowledge Attitude and Practice On Emergency Contraceptive Among Goba Female High School and Preparatory StudentsLawrence MungaPas encore d'évaluation
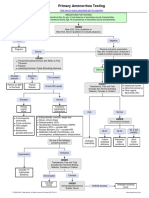
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiPas encore d'évaluation
- Vaginal Discharge + PruritisDocument56 pagesVaginal Discharge + PruritisEkoApriandhiPas encore d'évaluation
- Ob Review QuestionsDocument31 pagesOb Review QuestionsRandyPas encore d'évaluation
- STD - Infection That Are Passed From One Person To Another Through Sexual Contact. The Causes of StdsDocument3 pagesSTD - Infection That Are Passed From One Person To Another Through Sexual Contact. The Causes of StdsAngela BeatricePas encore d'évaluation
- Sexual Energy Control TechniqueDocument4 pagesSexual Energy Control Techniquesulya200483% (6)
- Sexual IntercourseDocument26 pagesSexual Intercoursenathan100% (2)
- Vajikarana KSRPrasadDocument36 pagesVajikarana KSRPrasadksr prasad100% (2)
- Reasons For Sexual Promiscuity in Chemically Dependent Respondents and Their Awareness and Acceptance of Condom UseDocument7 pagesReasons For Sexual Promiscuity in Chemically Dependent Respondents and Their Awareness and Acceptance of Condom UsestarscribPas encore d'évaluation
- Normoz TabletDocument6 pagesNormoz TabletAmita VermaPas encore d'évaluation