Vous aimerez peut-être aussi
- Enrolment FormDocument2 pagesEnrolment Formapi-291451017Pas encore d'évaluation
- Sarv Suraksha Claim Form 111Document3 pagesSarv Suraksha Claim Form 111ritikarustogiPas encore d'évaluation
- Claimant Statement Form Death Claim 2Document3 pagesClaimant Statement Form Death Claim 2Anitha AnuPas encore d'évaluation
- Annexure A - Candidate Information Declaration FormDocument7 pagesAnnexure A - Candidate Information Declaration FormS Kamble100% (1)
- PDF-PO ID Cards Application FormDocument2 pagesPDF-PO ID Cards Application FormSriteja Josyula100% (1)
- Pmsby Forms - RevisedDocument9 pagesPmsby Forms - RevisedSakareSreenivasPas encore d'évaluation
- Aadhaar Enrolment Form - 21042012Document1 pageAadhaar Enrolment Form - 21042012Abhinay Gajula50% (8)
- ConsentDocument3 pagesConsentMduduzi Magiva MahlanguPas encore d'évaluation
- Enrolment Form AadharDocument2 pagesEnrolment Form AadhardrmohangPas encore d'évaluation
- 1.reimbursement Claim FormDocument3 pages1.reimbursement Claim FormVijiPas encore d'évaluation
- Claim FormDocument2 pagesClaim FormsrikanthPas encore d'évaluation
- New Claim Form TTK TPADocument2 pagesNew Claim Form TTK TPAAbhijit SawantPas encore d'évaluation
- Please Read The Instructions Carefully Before You Fill Form 10 CDocument6 pagesPlease Read The Instructions Carefully Before You Fill Form 10 CVishal PadiyarPas encore d'évaluation
- Aadhaar Enrolment Correction Form Version 2.1Document2 pagesAadhaar Enrolment Correction Form Version 2.1makPas encore d'évaluation
- Aadhaar Enrolment Correction Form Version 2.1Document2 pagesAadhaar Enrolment Correction Form Version 2.1Saravanan ShankarPas encore d'évaluation
- Aadhaar Enrolment/ Correction/ Update FormDocument2 pagesAadhaar Enrolment/ Correction/ Update FormasasasasasPas encore d'évaluation
- Death Claimant StatementDocument4 pagesDeath Claimant Statementcet.ranchi7024Pas encore d'évaluation
- Aadhaar Enrolment Correction Form Version 2.1Document2 pagesAadhaar Enrolment Correction Form Version 2.1Aman BediPas encore d'évaluation
- Aadhaar Enrolment Form Filling GuideDocument2 pagesAadhaar Enrolment Form Filling GuideChandra Pratap ChauhanPas encore d'évaluation
- Aadhar Enrolment Correction FormDocument2 pagesAadhar Enrolment Correction Formapi-249989744Pas encore d'évaluation
- Aadhaar Enrolment Correction Form Version 4.0Document2 pagesAadhaar Enrolment Correction Form Version 4.0Ansar AliPas encore d'évaluation
- Claim FormDocument4 pagesClaim Formprashant pawarPas encore d'évaluation
- The Oriental Insurance Company LimitedDocument5 pagesThe Oriental Insurance Company LimitedRaviJhaPas encore d'évaluation
- Death Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3Document3 pagesDeath Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3vertine belerPas encore d'évaluation
- Bajaj Allianz General Insurance Company Limited: Overseas Travel Insurance Claim FormDocument4 pagesBajaj Allianz General Insurance Company Limited: Overseas Travel Insurance Claim FormSumitPas encore d'évaluation
- Aadhaar Enrolment Correction Form Version 2.1Document2 pagesAadhaar Enrolment Correction Form Version 2.1ashish50% (2)
- Claim Form For Deceased VictimsDocument3 pagesClaim Form For Deceased VictimsMichael_Lee_RobertsPas encore d'évaluation
- Adhhar Application FarmDocument2 pagesAdhhar Application FarmjaigodaraPas encore d'évaluation
- 0811 Ma App Form Version 190 1Document3 pages0811 Ma App Form Version 190 1vmjjc7jtg2Pas encore d'évaluation
- General Instructions - Wipro Bps Eoffer: Eonboarding Via Remote Document UploadDocument3 pagesGeneral Instructions - Wipro Bps Eoffer: Eonboarding Via Remote Document UploadEllaboina KalyaniPas encore d'évaluation
- HRSSSC Anexure For JEDocument8 pagesHRSSSC Anexure For JEAbhishekPas encore d'évaluation
- 1378 - 1 - 1 - All Anexure PDFDocument8 pages1378 - 1 - 1 - All Anexure PDFprashant guptaPas encore d'évaluation
- Form 60: VerificationDocument8 pagesForm 60: VerificationJeetender KumarPas encore d'évaluation
- Global Filipino Money Card Application Form: Exhibit 4Document1 pageGlobal Filipino Money Card Application Form: Exhibit 4아베죠반Pas encore d'évaluation
- Pmsby 2Document7 pagesPmsby 2Amit BhardwajPas encore d'évaluation
- Aadhaar Enrolment Correction Form Version 2.1Document1 pageAadhaar Enrolment Correction Form Version 2.1nagasaigoparajuPas encore d'évaluation
- 070123-PAI & AAI Claim FormsDocument6 pages070123-PAI & AAI Claim FormsVikas Singh ChandelPas encore d'évaluation
- Annexure A - Candidate Information Declaration FormDocument7 pagesAnnexure A - Candidate Information Declaration FormS KamblePas encore d'évaluation
- Tata-Aig General Insurance Company LTD: Policy No. 0238443404 / 0238443469 Claim No.Document3 pagesTata-Aig General Insurance Company LTD: Policy No. 0238443404 / 0238443469 Claim No.Mahendra SinghPas encore d'évaluation
- Annexure A - Applicant Information & Declaration FormDocument8 pagesAnnexure A - Applicant Information & Declaration FormAnonymous rYZyQQot55Pas encore d'évaluation
- Report of Medical Examination and Vaccination RecordDocument14 pagesReport of Medical Examination and Vaccination RecordHrishi WaghPas encore d'évaluation
- Aa1896352985985172822158 S.joshuaDocument8 pagesAa1896352985985172822158 S.joshuaprabhu768Pas encore d'évaluation
- Health Insurance Claim Form GuideDocument3 pagesHealth Insurance Claim Form GuideEkta ChauhanPas encore d'évaluation
- Enrollment Card For Group Insurance: Member InformationDocument1 pageEnrollment Card For Group Insurance: Member Informationsue annePas encore d'évaluation
- SSSForm ACOP Form Certified OfficialDocument3 pagesSSSForm ACOP Form Certified Officialmcad_mariePas encore d'évaluation
- AFP Form Manual - 10 Oct 2016Document2 pagesAFP Form Manual - 10 Oct 2016sppramPas encore d'évaluation
- w-6 Player Personnel From 1Document1 pagew-6 Player Personnel From 1api-318868438Pas encore d'évaluation
- Formats Pensioners NHIS 2014Document4 pagesFormats Pensioners NHIS 2014Raj RudrapaaPas encore d'évaluation
- Motor Claim FormDocument2 pagesMotor Claim Formjqspkid166Pas encore d'évaluation
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsD'EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsÉvaluation : 4.5 sur 5 étoiles4.5/5 (12)
- US Immigration Exam Study Guide in English and Albanian: Study Guides for the US Immigration TestD'EverandUS Immigration Exam Study Guide in English and Albanian: Study Guides for the US Immigration TestPas encore d'évaluation
- Immigration: A Fiance Petition Document Preparation Reference.D'EverandImmigration: A Fiance Petition Document Preparation Reference.Pas encore d'évaluation
- Innocent Spouse Relief: How You May Not Have To Pay Your Taxes!D'EverandInnocent Spouse Relief: How You May Not Have To Pay Your Taxes!Pas encore d'évaluation
- Stop Bill Collectors: The No Bull Guide to Outwitting Bill CollectorsD'EverandStop Bill Collectors: The No Bull Guide to Outwitting Bill CollectorsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Sujit Kumar Rout, Rupashree Ragini Sahoo, Soumya Ranjan Satapathy, Barada Prasad SethyDocument7 pagesSujit Kumar Rout, Rupashree Ragini Sahoo, Soumya Ranjan Satapathy, Barada Prasad SethyPrabu ThannasiPas encore d'évaluation
- Task and Link Analysis AssignmentDocument4 pagesTask and Link Analysis AssignmentAzeem NawazPas encore d'évaluation
- Logistic RegressionDocument17 pagesLogistic RegressionLovedeep Chaudhary100% (1)
- Rajani Panchal Phone: - 0279642567Document4 pagesRajani Panchal Phone: - 0279642567Phillip JohnsonPas encore d'évaluation
- Ceramic Tiles Industry Research ProjectDocument147 pagesCeramic Tiles Industry Research Projectsrp188Pas encore d'évaluation
- The Minecraft Survival Quest ChallengeDocument4 pagesThe Minecraft Survival Quest Challengeapi-269630780100% (1)
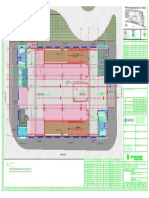
- Key plan and area statement comparison for multi-level car park (MLCPDocument1 pageKey plan and area statement comparison for multi-level car park (MLCP121715502003 BOLLEMPALLI BINDU SREE SATYAPas encore d'évaluation
- STTH2002C: High Efficiency Ultrafast DiodeDocument16 pagesSTTH2002C: High Efficiency Ultrafast DiodeAseng saputraPas encore d'évaluation
- Newman News January 2017 EditionDocument12 pagesNewman News January 2017 EditionSonya MathesonPas encore d'évaluation
- English Assignment AnswersDocument4 pagesEnglish Assignment AnswersAfidaPas encore d'évaluation
- The International Journal of Periodontics & Restorative DentistryDocument7 pagesThe International Journal of Periodontics & Restorative DentistrytaniaPas encore d'évaluation
- Unit 6 ( CONSTRUCTION OF THE FLEXIBLE PAVEMENT )Document19 pagesUnit 6 ( CONSTRUCTION OF THE FLEXIBLE PAVEMENT )Zara Nabilah87% (15)
- Using Social Stories With Students With Social Emotional and Behavioral Disabilities The Promise and The Perils (2019)Document17 pagesUsing Social Stories With Students With Social Emotional and Behavioral Disabilities The Promise and The Perils (2019)SarahPas encore d'évaluation
- Martek Navgard BnwasDocument4 pagesMartek Navgard BnwasСергей БородинPas encore d'évaluation
- SteroidsDocument2 pagesSteroidsShawn FreemanPas encore d'évaluation
- Small-Scale Fisheries Co-op ConstitutionDocument37 pagesSmall-Scale Fisheries Co-op ConstitutionCalyn MusondaPas encore d'évaluation
- Automotive Relay PDFDocument3 pagesAutomotive Relay PDFSimon MclennanPas encore d'évaluation
- Online Dispute ResolutionDocument18 pagesOnline Dispute ResolutionMak YabuPas encore d'évaluation
- L10: Factors that Affect a Pendulum's PeriodDocument9 pagesL10: Factors that Affect a Pendulum's PeriodHeide CarrionPas encore d'évaluation
- FS 1 Observations of Teaching-Learning in Actual School EnvironmentDocument8 pagesFS 1 Observations of Teaching-Learning in Actual School EnvironmentJessie PeraltaPas encore d'évaluation
- H. P. Lovecraft - The Music of Erich ZannDocument14 pagesH. P. Lovecraft - The Music of Erich ZannMarco BologniniPas encore d'évaluation
- Catalogo Bombas PedrolloDocument80 pagesCatalogo Bombas PedrolloChesster EscobarPas encore d'évaluation
- Accenture Faq For New JoinersDocument4 pagesAccenture Faq For New JoinersBaazinow Hack Brainbaazi Live AnswersPas encore d'évaluation
- Hevc StandardDocument11 pagesHevc Standardganesh gangatharanPas encore d'évaluation
- MicroProcessadores ZelenovskyDocument186 pagesMicroProcessadores ZelenovskyDavid SantosPas encore d'évaluation
- Transforming City Governments For Successful Smart CitiesDocument194 pagesTransforming City Governments For Successful Smart CitiesTri Ramdani100% (2)
- Tutorial Letter 101/3/2018: Internal Auditing: Theory & PrinciplesDocument39 pagesTutorial Letter 101/3/2018: Internal Auditing: Theory & PrinciplesSAMANTHAPas encore d'évaluation
- Essential Components of an Effective Road Drainage SystemDocument11 pagesEssential Components of an Effective Road Drainage SystemRaisanAlcebarPas encore d'évaluation
- Return On Marketing InvestmentDocument16 pagesReturn On Marketing Investmentraj_thanviPas encore d'évaluation
- Engineering Standard for Rolling Stock Minimum In-Service ConditionsDocument19 pagesEngineering Standard for Rolling Stock Minimum In-Service Conditions4493464Pas encore d'évaluation