Vous aimerez peut-être aussi
- MalunionDocument25 pagesMalunionmichaelPas encore d'évaluation
- God Healing WayDocument96 pagesGod Healing WayIrinaConstantin100% (1)
- ASA Guidelines For Sedation and AnalgesiaDocument14 pagesASA Guidelines For Sedation and AnalgesiamichaelPas encore d'évaluation
- PheochromocytomaDocument74 pagesPheochromocytomamichaelPas encore d'évaluation
- Anesthesia Management For Laparoscpic SurgeryDocument33 pagesAnesthesia Management For Laparoscpic Surgerymichael0% (1)
- Monitored Anesthesia CareDocument22 pagesMonitored Anesthesia Caremichael100% (4)
- Bradycardia During Induction of Anesthesia WithDocument21 pagesBradycardia During Induction of Anesthesia WithmichaelPas encore d'évaluation
- Intravenous Technique in Ambulatory AnesthesiaDocument16 pagesIntravenous Technique in Ambulatory AnesthesiamichaelPas encore d'évaluation
- Anesthetic Considerations for Outpatient ColonoscopyDocument24 pagesAnesthetic Considerations for Outpatient ColonoscopymichaelPas encore d'évaluation
- Schizophrenia: 2 Most Frequent Diagnosis of Patients 14-64 Y/o at CRH in 2008Document52 pagesSchizophrenia: 2 Most Frequent Diagnosis of Patients 14-64 Y/o at CRH in 2008michaelPas encore d'évaluation
- Anatomy and Physiology of the Cardiovascular SystemDocument55 pagesAnatomy and Physiology of the Cardiovascular SystemPrabhjeet Kaur SainiPas encore d'évaluation
- Pediatric AnesthesiaDocument33 pagesPediatric AnesthesiamichaelPas encore d'évaluation
- Anatomy of The LarynxDocument41 pagesAnatomy of The LarynxmichaelPas encore d'évaluation
- Cardiovascular PhysiologyDocument35 pagesCardiovascular PhysiologyLuiz Jorge MendonçaPas encore d'évaluation
- Bradycardia During Induction of Anesthesia WithDocument21 pagesBradycardia During Induction of Anesthesia WithmichaelPas encore d'évaluation
- Obstetric Emergency and Anesthetic ManagementDocument11 pagesObstetric Emergency and Anesthetic ManagementmichaelPas encore d'évaluation
- CV Anatomy and PhysiologyDocument24 pagesCV Anatomy and PhysiologymichaelPas encore d'évaluation
- Pediatric AnesthesiaDocument15 pagesPediatric Anesthesiamichael100% (6)
- CV AnatomyDocument49 pagesCV AnatomymichaelPas encore d'évaluation
- Airway Management WordDocument2 pagesAirway Management WordmichaelPas encore d'évaluation
- Inhalation Anesthesia WordsDocument2 pagesInhalation Anesthesia WordsmichaelPas encore d'évaluation
- Fluids and ElectrolyteDocument83 pagesFluids and ElectrolytemichaelPas encore d'évaluation
- Anesthetic MachineDocument80 pagesAnesthetic MachinemichaelPas encore d'évaluation
- Bradycardia During Induction of Anesthesia WithDocument21 pagesBradycardia During Induction of Anesthesia WithmichaelPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5782)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Synapse StructureDocument34 pagesSynapse Structuredr_mohanad100% (1)
- The Effect of Caffeine On Cognitive FunctionsDocument4 pagesThe Effect of Caffeine On Cognitive FunctionsCliff KaaraPas encore d'évaluation
- Cholinergic DrugsDocument11 pagesCholinergic Drugsshivanshpande100% (1)
- Dimerization of G-Protein Coupled Receptors: Mechanisms and Functional ConsequencesDocument11 pagesDimerization of G-Protein Coupled Receptors: Mechanisms and Functional ConsequencesKristoffer SagbraatenPas encore d'évaluation
- The Hitchhiker's Guide To Clinical Pharmacology: Pharmacodynamics: How Drugs WorkDocument23 pagesThe Hitchhiker's Guide To Clinical Pharmacology: Pharmacodynamics: How Drugs WorkMylz MendozaPas encore d'évaluation
- Acetylcholine ReceptorDocument1 pageAcetylcholine Receptorsai calderPas encore d'évaluation
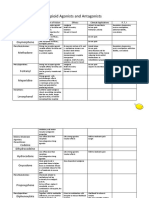
- Opioid Agonists and AntagonistsDocument5 pagesOpioid Agonists and AntagonistsCas BuPas encore d'évaluation
- Antihistamine - WikipediaDocument39 pagesAntihistamine - WikipediaMuhammadafif SholehuddinPas encore d'évaluation
- The Effects of Trazodone on Young and Old Animals After StrokeDocument1 pageThe Effects of Trazodone on Young and Old Animals After StrokeRezidentiat UmfPas encore d'évaluation
- Science:, 1870 (1999) Robert C. Malenka and and Roger A. NicollDocument6 pagesScience:, 1870 (1999) Robert C. Malenka and and Roger A. NicollMaría Celeste Sánchez SugíaPas encore d'évaluation
- Apoptosis Pathway 1Document2 pagesApoptosis Pathway 1Dharmendra SinghPas encore d'évaluation
- NeurotransmittersDocument36 pagesNeurotransmittersDr. M. Prasad NaiduPas encore d'évaluation
- Biology - May 2017Document1 pageBiology - May 2017Rahique ShuaibPas encore d'évaluation
- PDFDocument238 pagesPDFGiorgiDanelyanPas encore d'évaluation
- 2 PHAR0004 9 7 ReceptorStructure NSM 2018 NotesDocument3 pages2 PHAR0004 9 7 ReceptorStructure NSM 2018 NotesArthi ArumukasamyPas encore d'évaluation
- Neurotransmitter 2Document23 pagesNeurotransmitter 2VIKAS PUNIAPas encore d'évaluation
- 10 - Chapter - 4 PDFDocument163 pages10 - Chapter - 4 PDFBalakrishna GopinathPas encore d'évaluation
- Chapter 3 - Cell Signaling and Endocrine RegulationDocument75 pagesChapter 3 - Cell Signaling and Endocrine RegulationDee Buendia100% (1)
- Cell Signaling Write UpDocument4 pagesCell Signaling Write Upinfinity chronusPas encore d'évaluation
- The Endocannabinoid System As It Relates To AutismDocument16 pagesThe Endocannabinoid System As It Relates To AutismUPMMJ100% (3)
- SIGNAL TRANSDUCTION PATHWAYSDocument38 pagesSIGNAL TRANSDUCTION PATHWAYSIndraPramanaIdaBagusPas encore d'évaluation
- Sympathetic Agonist and Antagonist 23Document12 pagesSympathetic Agonist and Antagonist 23PPas encore d'évaluation
- Drug Receptor InteractionDocument29 pagesDrug Receptor InteractionFaisal RahmanPas encore d'évaluation
- B22 Neural Mechanisms of Learning & MemoryDocument21 pagesB22 Neural Mechanisms of Learning & MemoryNilanjana Chatterjee ChakrabortyPas encore d'évaluation
- Chemistry-Viii Notes Prepared by Dr. Dhondiba Vishwanath Suryawanshi, GFGC KR Puram Bengaluru-36Document9 pagesChemistry-Viii Notes Prepared by Dr. Dhondiba Vishwanath Suryawanshi, GFGC KR Puram Bengaluru-36Dr. Dhondiba Vishwanath0% (1)
- Dog ED Signaling Case Study-2Document3 pagesDog ED Signaling Case Study-2Pingu BossPas encore d'évaluation
- Psychopharmacology Drugs, The Brain, and BehaviorDocument13 pagesPsychopharmacology Drugs, The Brain, and Behavior陳琮方5% (21)
- NPB 100 Midterm 1 Study Guide-1Document4 pagesNPB 100 Midterm 1 Study Guide-1April MartínezPas encore d'évaluation
- Neurology and Special Senses ' Neurology and Special Senses ' Section IiiDocument20 pagesNeurology and Special Senses ' Neurology and Special Senses ' Section IiiLuis Jose VelazquezPas encore d'évaluation
- Action Potential MOST RECENT Ch48 - Accessible - Lecture - PresentationDocument81 pagesAction Potential MOST RECENT Ch48 - Accessible - Lecture - PresentationSallyPas encore d'évaluation