Vous aimerez peut-être aussi
- Artigo - Factors in Risk PerceptionDocument11 pagesArtigo - Factors in Risk PerceptionRicardo GomesPas encore d'évaluation
- Arcgis Help 10.1: Tutorial: Publishing A Map ServiceDocument1 pageArcgis Help 10.1: Tutorial: Publishing A Map ServiceRicardo GomesPas encore d'évaluation
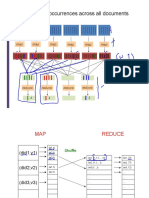
- 017 Map Reduce AbstractionDocument61 pages017 Map Reduce AbstractionRicardo GomesPas encore d'évaluation
- 4.1 Common Statistical Tests and Applications in Epidemiological LiteratureDocument6 pages4.1 Common Statistical Tests and Applications in Epidemiological LiteratureRicardo GomesPas encore d'évaluation
- Week 3 Epi Tool KitDocument2 pagesWeek 3 Epi Tool KitRicardo GomesPas encore d'évaluation
- 3.4 Cross-Sectional StudiesDocument4 pages3.4 Cross-Sectional StudiesRicardo Gomes100% (1)
- 3.3 Case-Control StudiesDocument5 pages3.3 Case-Control StudiesRicardo GomesPas encore d'évaluation
- Tutorial SemivarDocument16 pagesTutorial SemivarRicardo GomesPas encore d'évaluation
- Tutorial SpatialDocument19 pagesTutorial SpatialRicardo GomesPas encore d'évaluation
- Week 2 Epi Tool KitDocument1 pageWeek 2 Epi Tool KitRicardo GomesPas encore d'évaluation
- Tutorial OKDocument12 pagesTutorial OKRicardo GomesPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Multi Phase Flow in WellDocument149 pagesMulti Phase Flow in WellOmar 'Tanzania'100% (1)
- 27-12-14 SR - Iit-Z (Iz) Co-Spark Jee Main (2011) Ptm-16 Q'paperDocument23 pages27-12-14 SR - Iit-Z (Iz) Co-Spark Jee Main (2011) Ptm-16 Q'paperazeemPas encore d'évaluation
- Lutensol TO Types: Technical InformationDocument15 pagesLutensol TO Types: Technical InformationLjupco AleksovPas encore d'évaluation
- Jenway 74 76 Series BrochureDocument6 pagesJenway 74 76 Series BrochureSadik OunisPas encore d'évaluation
- Isolated Phase Bus Inspection & Maintenance Best Practices: Mohsen Tarassoly Electrical Builders, Inc. (EBI)Document50 pagesIsolated Phase Bus Inspection & Maintenance Best Practices: Mohsen Tarassoly Electrical Builders, Inc. (EBI)bobyPas encore d'évaluation
- Plastic MaterialDocument8 pagesPlastic MaterialSenthil Kumar GanesanPas encore d'évaluation
- Experimestnt 1 (Structure Lab)Document32 pagesExperimestnt 1 (Structure Lab)AZem AziZi Mirza50% (2)
- Pengaruh Kandungan Frekuensi Gempa Terhadap Simpangan Dan Drift Ratio 2 Arah Struktur Bangunan Set-Back Bertingkat BanyakDocument9 pagesPengaruh Kandungan Frekuensi Gempa Terhadap Simpangan Dan Drift Ratio 2 Arah Struktur Bangunan Set-Back Bertingkat BanyakIvan MuhammadPas encore d'évaluation
- 2nd Year Math Guess PaperDocument6 pages2nd Year Math Guess PaperArmaan MalikPas encore d'évaluation
- 1.8 Rack Shift of The Gear: UndercutDocument6 pages1.8 Rack Shift of The Gear: UndercutJuanPas encore d'évaluation
- Bryton Williamson - Percent - Composition PracticeDocument2 pagesBryton Williamson - Percent - Composition PracticeBryton WilliamsonPas encore d'évaluation
- A Review of Piezoelectric Energy Harvesting Based On VibrationDocument13 pagesA Review of Piezoelectric Energy Harvesting Based On VibrationardnetirarhsimPas encore d'évaluation
- Se Single Phase Inverter DatasheetDocument2 pagesSe Single Phase Inverter DatasheetsabrahimaPas encore d'évaluation
- Payable Salary Paid SalaryDocument2 pagesPayable Salary Paid SalaryAhmed AmmanPas encore d'évaluation
- Building Envelope Design Guide - Curtain Walls - Whole Building Design GuideDocument8 pagesBuilding Envelope Design Guide - Curtain Walls - Whole Building Design GuideAyman_Elmasry_9107Pas encore d'évaluation
- Impulse Response of Frequency Domain ComponentDocument17 pagesImpulse Response of Frequency Domain Componentbubo28Pas encore d'évaluation
- Cambridge IGCSE: MATHEMATICS 0580/42Document20 pagesCambridge IGCSE: MATHEMATICS 0580/42spotifysubs250Pas encore d'évaluation
- SOALAN BiologiDocument12 pagesSOALAN BiologiLoong Wai FamPas encore d'évaluation
- 4.3 Forced WavesDocument23 pages4.3 Forced WavesPritib KumarPas encore d'évaluation
- CS3205 A8Document10 pagesCS3205 A8Rian BattlaxPas encore d'évaluation
- Nitro Shock AbsorbersDocument18 pagesNitro Shock AbsorbersPavan KumarPas encore d'évaluation
- Face Detection RecognitionDocument21 pagesFace Detection RecognitionkamendersinghgangwarPas encore d'évaluation
- Seminar On Wireless Charging of Mobile DevicesDocument24 pagesSeminar On Wireless Charging of Mobile DevicesGourish Amonkar100% (1)
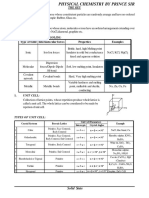
- Etoos Solid State PS SirDocument27 pagesEtoos Solid State PS SirGyandeep KalitaPas encore d'évaluation
- Sorge 2015Document18 pagesSorge 2015Masih LoghmaniPas encore d'évaluation
- Chapter 7 Powerpoint 1225339266570076 9Document24 pagesChapter 7 Powerpoint 1225339266570076 9venkateshyadav2116Pas encore d'évaluation
- Mills - CatalogDocument4 pagesMills - Catalogdéborah_rosalesPas encore d'évaluation
- Hamerlug Unions (Anson)Document15 pagesHamerlug Unions (Anson)Leonardo ViannaPas encore d'évaluation
- Effect of Specimen Thickness and Stress Ratio On Fatigue Crack Growth After A Single Overload Cycle On Structural SteelDocument8 pagesEffect of Specimen Thickness and Stress Ratio On Fatigue Crack Growth After A Single Overload Cycle On Structural SteelKamal MankariPas encore d'évaluation
- Neodymium MagnetDocument42 pagesNeodymium MagnetpraveenPas encore d'évaluation