Vous aimerez peut-être aussi
- Importance of EmotionsDocument3 pagesImportance of EmotionsnatahondriaPas encore d'évaluation
- Mnemonics Anatomy 1st SemDocument4 pagesMnemonics Anatomy 1st SemNastassja Callmedoctor Douse67% (3)
- Anatomy and Physiology of Adrenal GlandDocument26 pagesAnatomy and Physiology of Adrenal GlandYAMINIPRIYANPas encore d'évaluation
- HydrocephalusDocument21 pagesHydrocephalusprecillathoppil100% (2)
- 16 Respiratory AlkalosisDocument28 pages16 Respiratory AlkalosisJoel Topf100% (2)
- PartoghraphDocument60 pagesPartoghraphharley dela cruzPas encore d'évaluation
- Sepak Takraw Training ProgramDocument1 pageSepak Takraw Training ProgramMarston Glenn Tugahan100% (3)
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocument31 pagesNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanPas encore d'évaluation
- Hematological Alterations: Disseminated Intravascular Coagulation (DIC)Document16 pagesHematological Alterations: Disseminated Intravascular Coagulation (DIC)jhommmmmPas encore d'évaluation
- Hepatic Encephalopathy: Causes, Tests, and Treatment OptionsD'EverandHepatic Encephalopathy: Causes, Tests, and Treatment OptionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Care of Client in Mechanical VentilatorDocument11 pagesCare of Client in Mechanical VentilatorVignesh Viggy100% (4)
- Dyspnea: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingDocument19 pagesDyspnea: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingNaseem Bin YoosafPas encore d'évaluation
- Standard Precautions in Infection ControlDocument8 pagesStandard Precautions in Infection ControlAkshaya Mistry100% (1)
- Disseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandDisseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Unconsciousness: Anil PatidarDocument29 pagesUnconsciousness: Anil Patidarjinal sutharPas encore d'évaluation
- Framework. Scope and Trends in Nursing PracticeDocument60 pagesFramework. Scope and Trends in Nursing PracticeShaells Joshi50% (2)
- Models of PreventionDocument21 pagesModels of Preventionprecillathoppil100% (5)
- Daniel N. Stern MD: OxfordDocument22 pagesDaniel N. Stern MD: OxfordGEMA PAEZ LOBOSPas encore d'évaluation
- Acute Respiratory Distress Syndrome (ARDS) : MR Sanjay. M. Peerapur, Principal, KLES Institute of Nursing Sciences, HubliDocument22 pagesAcute Respiratory Distress Syndrome (ARDS) : MR Sanjay. M. Peerapur, Principal, KLES Institute of Nursing Sciences, Hublimanish dafdaPas encore d'évaluation
- Health Assessment of Bronchial Asthma PatientDocument3 pagesHealth Assessment of Bronchial Asthma PatientShetal SharmaPas encore d'évaluation
- Skill Laboratory Practice Module: Block: Reproductive System: 10 Topic: Pap SmearDocument5 pagesSkill Laboratory Practice Module: Block: Reproductive System: 10 Topic: Pap SmearMuthiana Rizky0% (1)
- Teaching Deep Breathing and Coughing ExercisesDocument5 pagesTeaching Deep Breathing and Coughing ExercisesBianx Flores DosdosPas encore d'évaluation
- Exchange Blood Transfusion 2Document15 pagesExchange Blood Transfusion 2Sarah100% (1)
- Lung AbscessDocument46 pagesLung AbscessJeevitha VanithaPas encore d'évaluation
- Management of Stoma, Cut and WoundsDocument40 pagesManagement of Stoma, Cut and WoundsLalita KumariPas encore d'évaluation
- Tetralogy of FallotDocument10 pagesTetralogy of FallotanggiehardiyantiPas encore d'évaluation
- Ventilation Long Term ChildDocument58 pagesVentilation Long Term ChildstarykPas encore d'évaluation
- NasoGastric Tube FeedingDocument3 pagesNasoGastric Tube FeedingSwati SharmaPas encore d'évaluation
- Emergency Acupressure TreatmentDocument39 pagesEmergency Acupressure TreatmentNarayana Mugalur100% (1)
- Cardio Pulmonary Resuscitation and End of Life CareDocument22 pagesCardio Pulmonary Resuscitation and End of Life CareAnitha sujithPas encore d'évaluation
- Management of ARDSDocument57 pagesManagement of ARDSRajaPas encore d'évaluation
- Lymphoma in ChildrenDocument42 pagesLymphoma in ChildrenPriyaPas encore d'évaluation
- Av Aids FinalDocument17 pagesAv Aids Finalprecillathoppil0% (1)
- AARC Clinical Practice Guideline: Incentive SpirometryDocument10 pagesAARC Clinical Practice Guideline: Incentive SpirometrytruptimptPas encore d'évaluation
- Guidance & CounsellingDocument16 pagesGuidance & Counsellingprecillathoppil75% (8)
- Icu Equipments BY: Presented Bhupender Kumar MehtoDocument35 pagesIcu Equipments BY: Presented Bhupender Kumar Mehtobhupendermehto012Pas encore d'évaluation
- CURRENT STATUS OF CHILD HEALTH IN INDIA To Be PrintDocument6 pagesCURRENT STATUS OF CHILD HEALTH IN INDIA To Be Printprecillathoppil96% (24)
- Major Neurological Syndromes PDFDocument260 pagesMajor Neurological Syndromes PDFVirlan Vasile Catalin100% (1)
- Current Trends in Nursing Educaion..MadhuDocument13 pagesCurrent Trends in Nursing Educaion..Madhuprecillathoppil100% (1)
- Course PlANDocument7 pagesCourse PlANprecillathoppil50% (4)
- Critical Care UnitsDocument25 pagesCritical Care UnitsJaya Prabha100% (2)
- History and Physical Assessment of Integumentary System: By: Mr. M - Shiva Nanda ReddyDocument84 pagesHistory and Physical Assessment of Integumentary System: By: Mr. M - Shiva Nanda ReddyNilakshi Barik MandalPas encore d'évaluation
- Hiv and Aids in ChildrenDocument36 pagesHiv and Aids in ChildrenKazau FwalangaPas encore d'évaluation
- PneumothoraxDocument3 pagesPneumothoraxSanthosh.S.UPas encore d'évaluation
- Cardiopulmonary Cerebral ResuscitationDocument17 pagesCardiopulmonary Cerebral ResuscitationrizalPas encore d'évaluation
- Rheumatic Fever and RHDDocument49 pagesRheumatic Fever and RHDbereket gashuPas encore d'évaluation
- National Control of Dirrheal Diseases (CDD) Program ObjectivesDocument6 pagesNational Control of Dirrheal Diseases (CDD) Program ObjectivesJoy FucananPas encore d'évaluation
- Cpms College of Nursing: Assignment ON Colonic IrrigationDocument3 pagesCpms College of Nursing: Assignment ON Colonic IrrigationAmy Lalringhluani ChhakchhuakPas encore d'évaluation
- Erythroblastosis Fetalis - AprilDocument2 pagesErythroblastosis Fetalis - AprilNurse April GonzalesPas encore d'évaluation
- Nursing Care PneumoniaDocument26 pagesNursing Care PneumoniaIsaac Kipkemoi100% (1)
- Care of Unconscious PatientDocument6 pagesCare of Unconscious PatientSuparna SinghaPas encore d'évaluation
- 5 Bleeding Disorders PPT EditedDocument87 pages5 Bleeding Disorders PPT EditedFrances Isabella OlasimanPas encore d'évaluation
- Hepatitis in ChildrenDocument2 pagesHepatitis in ChildrenShilpi SinghPas encore d'évaluation
- What Is ICU PsychosisDocument6 pagesWhat Is ICU PsychosisAngelicaMarieRafananPas encore d'évaluation
- Nursing Practice Standards2Document25 pagesNursing Practice Standards2sunielgowdaPas encore d'évaluation
- Laryngeal Cancer Powerpoint FinalllllDocument30 pagesLaryngeal Cancer Powerpoint Finalllllapi-396575125Pas encore d'évaluation
- Medical Surgical Nursing Suretech College of NursingDocument18 pagesMedical Surgical Nursing Suretech College of NursingSanket TelangPas encore d'évaluation
- NEONATAL APNOEA SMNRDocument18 pagesNEONATAL APNOEA SMNRAswathy RC100% (1)
- Certificate in Paediatric Nursing: ProgrammeDocument67 pagesCertificate in Paediatric Nursing: ProgrammeWOne WannPas encore d'évaluation
- Pulse Oximetry Practical ApplicationsDocument4 pagesPulse Oximetry Practical ApplicationsShauna Martin0% (1)
- Congenital Heart DiseaseDocument12 pagesCongenital Heart Diseaserakanootousan100% (1)
- Disorders of AortaDocument25 pagesDisorders of Aortavani reddyPas encore d'évaluation
- Central Venous PressureDocument10 pagesCentral Venous PressureAngelo ArquizaPas encore d'évaluation
- MeningitisDocument12 pagesMeningitisFaith Vaughn100% (2)
- Psychiatric EmergenciesDocument25 pagesPsychiatric EmergenciesAnnapurna DangetiPas encore d'évaluation
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress Syndromef.abrahamPas encore d'évaluation
- Health Problems MyselfDocument54 pagesHealth Problems MyselfKrishnaveni Murugesh100% (2)
- Modes of Mechanical Ventilation ADocument23 pagesModes of Mechanical Ventilation Anisha kaushikPas encore d'évaluation
- ETT IntubationDocument10 pagesETT IntubationPoova RagavanPas encore d'évaluation
- A Study To Assess The Effectiveness of Structure Teaching Programme On Knowledge Regarding Prevention of Childhood Accidents Among Mothers of Under Five Children at Piparia, Vadodara.Document8 pagesA Study To Assess The Effectiveness of Structure Teaching Programme On Knowledge Regarding Prevention of Childhood Accidents Among Mothers of Under Five Children at Piparia, Vadodara.International Organization of Scientific Research (IOSR)Pas encore d'évaluation
- BMTDocument44 pagesBMTGargi MPPas encore d'évaluation
- Management of Post Term PregnancyDocument11 pagesManagement of Post Term Pregnancyapi-3705046100% (3)
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathySuhas KandePas encore d'évaluation
- Anatomy & Physiology of The Eye, A ReviewDocument24 pagesAnatomy & Physiology of The Eye, A ReviewArnold DanielPas encore d'évaluation
- A Case Study On A Patient With TyphoidDocument43 pagesA Case Study On A Patient With TyphoidJef Sembrano DiplomaPas encore d'évaluation
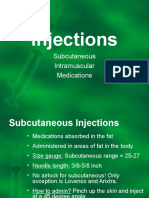
- Injections: Subcutaneous Intramuscular MedicationsDocument9 pagesInjections: Subcutaneous Intramuscular MedicationsprecillathoppilPas encore d'évaluation
- Visit To Nariniketan Jabalpur: 1. To Encourages Adoption of Orphans and Destitute Children. 2. 3. 4. 5. 6. 7Document7 pagesVisit To Nariniketan Jabalpur: 1. To Encourages Adoption of Orphans and Destitute Children. 2. 3. 4. 5. 6. 7precillathoppilPas encore d'évaluation
- PHPQ 6 X 8 SSDocument6 pagesPHPQ 6 X 8 SSprecillathoppilPas encore d'évaluation
- Master Rotatoin Plan M.SC Nursing 1st YearDocument2 pagesMaster Rotatoin Plan M.SC Nursing 1st YearprecillathoppilPas encore d'évaluation
- Principles of PreventionDocument14 pagesPrinciples of PreventionprecillathoppilPas encore d'évaluation
- Tutorial Lipid - AnswerDocument3 pagesTutorial Lipid - AnswerNida RidzuanPas encore d'évaluation
- Case 8 GUS - AKIDocument210 pagesCase 8 GUS - AKIGroup 12 Sofia HanaPas encore d'évaluation
- The Difficult or Failed Airway: Pat Melanson, MDDocument28 pagesThe Difficult or Failed Airway: Pat Melanson, MDMinorC3Pas encore d'évaluation
- Daftar PustakaDocument6 pagesDaftar Pustakaanon_791743164Pas encore d'évaluation
- Gonadal enDocument60 pagesGonadal enm7md TotiaPas encore d'évaluation
- Fluid Vol Deficit Secondary To Postpartum Hemorrhage Care PlanDocument3 pagesFluid Vol Deficit Secondary To Postpartum Hemorrhage Care PlanEllie GartungPas encore d'évaluation
- Neuroinflammatory Diseases: DR Okanga NDocument50 pagesNeuroinflammatory Diseases: DR Okanga NGladys MainaPas encore d'évaluation
- General Biology Q4 M3Document16 pagesGeneral Biology Q4 M3Delfin LeePas encore d'évaluation
- 7 MODULE 7 Nervous SystemDocument29 pages7 MODULE 7 Nervous SystemCHARIEMAE CA�AZARESPas encore d'évaluation
- Singh Et Al. 2022 - PCA - DescriptionDocument14 pagesSingh Et Al. 2022 - PCA - DescriptionFernanda SantosPas encore d'évaluation
- Respiratory SystemDocument27 pagesRespiratory Systemapi-210569514Pas encore d'évaluation
- Anatomy and Physiology of The BrainDocument2 pagesAnatomy and Physiology of The BrainkazellePas encore d'évaluation
- Common Med Surg Lab ValuesDocument5 pagesCommon Med Surg Lab ValuesToMorrowPas encore d'évaluation
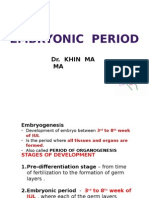
- Embryonic Period: Dr. Khin Ma MADocument34 pagesEmbryonic Period: Dr. Khin Ma MAIbrahim Foondun100% (1)
- Digital Vein ThrombosisDocument4 pagesDigital Vein ThrombosishestyPas encore d'évaluation
- Medical Entrance AIPMT PapersDocument15 pagesMedical Entrance AIPMT Paperssumit kumar0% (1)
- Biology Test: Plagiarism Grammar Technical Knowledge TotalDocument11 pagesBiology Test: Plagiarism Grammar Technical Knowledge Totalsonam snehaPas encore d'évaluation
- Bone McqsDocument4 pagesBone McqsAwan1994100% (2)
- Dna Replication, Translation, and TranscriptionDocument43 pagesDna Replication, Translation, and TranscriptionMaria VisitacionPas encore d'évaluation
- Fluids and ElectrolytesDocument49 pagesFluids and ElectrolytesvanessaPas encore d'évaluation
- ReflexesDocument7 pagesReflexesShaine Dominique SantosPas encore d'évaluation
- APPETITE: Physiological and Neurobiological AspectsDocument8 pagesAPPETITE: Physiological and Neurobiological AspectsTamara Souza RossiPas encore d'évaluation