Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- DFMEA of Bicycle SystemDocument2 pagesDFMEA of Bicycle SystemHarshan100% (5)
- Hybrid Athlete Program-1Document16 pagesHybrid Athlete Program-1Guilherme B.Ramos100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
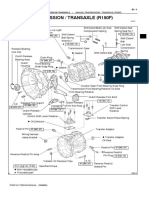
- Manual Transmission (R150F)Document3 pagesManual Transmission (R150F)daniel_gustavo_2002100% (4)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Young 1995 Lab Tests For StrengthDocument8 pagesYoung 1995 Lab Tests For Strengthmike.charlick3632100% (1)
- TCL Playing ConditionsDocument23 pagesTCL Playing ConditionsVinod KakyPas encore d'évaluation
- Qr25de PDFDocument216 pagesQr25de PDFJairo Rodriguez A.100% (2)
- Poems For Shared, Choral, Paired, and Echo Reading: Compiled byDocument38 pagesPoems For Shared, Choral, Paired, and Echo Reading: Compiled byDonna Rose O KeeneyPas encore d'évaluation
- Denso A4 EngineDocument18 pagesDenso A4 Enginefarid salmaniPas encore d'évaluation
- TURF FactionsDocument2 pagesTURF FactionsGiuseppe Di MartinoPas encore d'évaluation
- Fastner and Tooling Components. Fertrading Group Venezuela.Document4 pagesFastner and Tooling Components. Fertrading Group Venezuela.Renso PiovesanPas encore d'évaluation
- 2017 PPR Pipes PVC PlumbingDocument5 pages2017 PPR Pipes PVC PlumbingRichpaulPas encore d'évaluation
- Mahnidra XUV 700 BrochureDocument16 pagesMahnidra XUV 700 BrochuremsmotorindiaPas encore d'évaluation
- Great Dane 03chariot - PartscatalogDocument48 pagesGreat Dane 03chariot - Partscatalogcricket2654Pas encore d'évaluation
- Sports-Officiating Basketball VolleyballDocument24 pagesSports-Officiating Basketball Volleyballtrishia matasPas encore d'évaluation
- TOEFL-intro-paper-KEY (Complete Test Two-Pp269-292) PDFDocument1 pageTOEFL-intro-paper-KEY (Complete Test Two-Pp269-292) PDFSemjase ValAmPas encore d'évaluation
- PPE For PaintingDocument33 pagesPPE For PaintingdimasPas encore d'évaluation
- Legendary Monk FullDocument23 pagesLegendary Monk FullAnto MagaPas encore d'évaluation
- PUSH-UPPULL-UP New PlanDocument21 pagesPUSH-UPPULL-UP New Planvictor manuel100% (1)
- Case Study 2Document2 pagesCase Study 2LêĐức0% (1)
- Body Parts Lesson 1Document4 pagesBody Parts Lesson 1SusanaDelindroPas encore d'évaluation
- Organization and Management of Sports EventDocument4 pagesOrganization and Management of Sports EventErnan GuevarraPas encore d'évaluation
- About Me: Rassal Shaji 26 Male Ninny SunnyDocument10 pagesAbout Me: Rassal Shaji 26 Male Ninny SunnyRassal ShajiPas encore d'évaluation
- NewChallenges Workbook Level2 PDFDocument30 pagesNewChallenges Workbook Level2 PDFNatalia Astorga0% (1)
- The Player's Grimoire - Mage The AwakeningDocument35 pagesThe Player's Grimoire - Mage The Awakeningfinnia60050% (4)
- Scholastic Aptitude Test (SAT) : Answer Key NTSE Stage - II, 2019 (Test Date: 16 June. 2019)Document1 pageScholastic Aptitude Test (SAT) : Answer Key NTSE Stage - II, 2019 (Test Date: 16 June. 2019)Ravi RaviPas encore d'évaluation
- 2016natprisaa - Girls Team Final RankingDocument1 page2016natprisaa - Girls Team Final RankingCecilio AcasPas encore d'évaluation
- Repair Parts Sheet MIC-100, MIC-200/MC-75, MC-77: Mobile Crane UnitsDocument8 pagesRepair Parts Sheet MIC-100, MIC-200/MC-75, MC-77: Mobile Crane UnitsmecambPas encore d'évaluation
- Y-Puratek Telescoping Belt ConveyorDocument4 pagesY-Puratek Telescoping Belt ConveyorYousef AlipourPas encore d'évaluation
- Program OpeningsDocument2 pagesProgram OpeningsIliyan AleksievPas encore d'évaluation
- 2018 19 Mex f1 q0 Timing Qualifyingsessionmaximumspeeds v01Document1 page2018 19 Mex f1 q0 Timing Qualifyingsessionmaximumspeeds v01adeney_nickPas encore d'évaluation