Vous aimerez peut-être aussi
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesD'EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesÉvaluation : 4 sur 5 étoiles4/5 (2)
- Food & NutritionDocument21 pagesFood & NutritionSalman Preeom88% (24)
- Grade 11 Physical Education 1ST Periodical ExamDocument3 pagesGrade 11 Physical Education 1ST Periodical ExamJesus Austero100% (2)
- 99 Weight Loss Questions Answered 1 PDFDocument54 pages99 Weight Loss Questions Answered 1 PDFjasminePas encore d'évaluation
- Metabolic Syndrome: Denz Marc Ray T. Alea First Year ResidentDocument38 pagesMetabolic Syndrome: Denz Marc Ray T. Alea First Year ResidentDenz Marc Ray Alea100% (2)
- Adult Nutrition Guidelines For ICU PatientsDocument13 pagesAdult Nutrition Guidelines For ICU PatientsMariana MoralesPas encore d'évaluation
- 12 Week ShredDocument72 pages12 Week ShredSalvatore CalafiorePas encore d'évaluation
- 26 Golden Rules of Running EbookDocument37 pages26 Golden Rules of Running EbookPax AlquizaPas encore d'évaluation
- Am J Cardiol Deha EpaDocument10 pagesAm J Cardiol Deha EpajoremePas encore d'évaluation
- Metabolic Syndrome JhdjkwhekuhfdhjkewDocument48 pagesMetabolic Syndrome Jhdjkwhekuhfdhjkewkiki luhita sariPas encore d'évaluation
- To Eat or Not To Eat Dietary Fat in Uremia Is The QuestionDocument6 pagesTo Eat or Not To Eat Dietary Fat in Uremia Is The QuestionUriel FurlongPas encore d'évaluation
- Mekanisme Kerja Jurnal Alfa CyclodextrinDocument13 pagesMekanisme Kerja Jurnal Alfa CyclodextrinmonikaPas encore d'évaluation
- Medical Nutrition Therapy 4 Cardiovascular Disease April 2012-RevisiDocument66 pagesMedical Nutrition Therapy 4 Cardiovascular Disease April 2012-RevisiFachri Ihsan100% (1)
- Obesidade Rio de JaneiroDocument7 pagesObesidade Rio de JaneiroarianeoliPas encore d'évaluation
- Human Nutrition and MetabolismDocument6 pagesHuman Nutrition and MetabolismBruno CavicchioPas encore d'évaluation
- Jurnal DM-HFDDocument18 pagesJurnal DM-HFDLydya UtariPas encore d'évaluation
- Early Cardiac Changes in A Rat Model of Prediabetes: Brain Natriuretic Peptide Overexpression Seems To Be The Best MarkerDocument11 pagesEarly Cardiac Changes in A Rat Model of Prediabetes: Brain Natriuretic Peptide Overexpression Seems To Be The Best MarkerpopopioPas encore d'évaluation
- Nutrition in CVDsDocument37 pagesNutrition in CVDsRidhaPas encore d'évaluation
- Cardivascular Case Study 4Document57 pagesCardivascular Case Study 4api-302598263Pas encore d'évaluation
- Pres 3Document25 pagesPres 3api-262185461Pas encore d'évaluation
- CV Diet-Fk Modul 4.1 2015Document34 pagesCV Diet-Fk Modul 4.1 2015aryu.kusumastutiPas encore d'évaluation
- Nutritional Therapy For Cardiovascular DisorderDocument23 pagesNutritional Therapy For Cardiovascular DisordermatrixtrinityPas encore d'évaluation
- Canola 2Document11 pagesCanola 2Luis MesenPas encore d'évaluation
- Potent Antihypertensive Action of Dietary Flaxseed in Hypertensive PatientsDocument13 pagesPotent Antihypertensive Action of Dietary Flaxseed in Hypertensive PatientsMaRiana TorresPas encore d'évaluation
- 05 Hypertension 2009-1Document31 pages05 Hypertension 2009-1ajoshuaPas encore d'évaluation
- CVD Treatment Guidelines and MNTDocument94 pagesCVD Treatment Guidelines and MNTtecsoneckaPas encore d'évaluation
- Management of HyperlipidemiaDocument34 pagesManagement of HyperlipidemiaCarleta StanPas encore d'évaluation
- A Randomized Controlled Trial of The Effects of N 3 Fatty Acids On Resolvins in Chronic Kidney Disease - 2016 - Clinical NutritionDocument6 pagesA Randomized Controlled Trial of The Effects of N 3 Fatty Acids On Resolvins in Chronic Kidney Disease - 2016 - Clinical NutritionBby AdelinaPas encore d'évaluation
- High Intake of Saturated Fat, But Not Polyunsaturated Fat, Improves Survival in Heart Failure Despite Persistent Mitochondrial DefectsDocument9 pagesHigh Intake of Saturated Fat, But Not Polyunsaturated Fat, Improves Survival in Heart Failure Despite Persistent Mitochondrial DefectsRoger FaustinoPas encore d'évaluation
- Cardiovascular Disease - Kerala2Document77 pagesCardiovascular Disease - Kerala2Pradipta MukherjeePas encore d'évaluation
- L. Paci Fico, E. Bonci, M. Di Martino, P. Versacci, G. Andreoli, L.M. Silvestri, C. ChiesaDocument8 pagesL. Paci Fico, E. Bonci, M. Di Martino, P. Versacci, G. Andreoli, L.M. Silvestri, C. ChiesaDea PuspitaPas encore d'évaluation
- Nutrients 10 01385Document16 pagesNutrients 10 01385Alex GutiérrezPas encore d'évaluation
- Important Bioactive Properties of Omega-3 Fatty Acids: ReviewDocument7 pagesImportant Bioactive Properties of Omega-3 Fatty Acids: ReviewBao Chi Nguyen NgocPas encore d'évaluation
- Department of Medicine: Presented byDocument50 pagesDepartment of Medicine: Presented byArsh Surendra SinghPas encore d'évaluation
- Improving Cholesterol Profile Without Drugs: Yann A. Meunier, MD DirectorDocument51 pagesImproving Cholesterol Profile Without Drugs: Yann A. Meunier, MD Directorsadekar_sunil2804Pas encore d'évaluation
- Medical Nutrition Therapy For Cardiovascular Disease 2013Document30 pagesMedical Nutrition Therapy For Cardiovascular Disease 2013ashry909100% (1)
- Evans AgroFood Final 2011Document3 pagesEvans AgroFood Final 2011Joe EvansPas encore d'évaluation
- Rolul Alimentatiei Sanatoase in Prevenirea Diabetului ZaharatDocument33 pagesRolul Alimentatiei Sanatoase in Prevenirea Diabetului ZaharatDigei BobitzPas encore d'évaluation
- Lipidaholics Anonymous Case 291 Can Losing Weight Worsen Lipids?Document14 pagesLipidaholics Anonymous Case 291 Can Losing Weight Worsen Lipids?Edmilson R. LimaPas encore d'évaluation
- Obesity rp3Document7 pagesObesity rp3Dr Siddharth SP YadavPas encore d'évaluation
- Dyslipidemia 2018Document8 pagesDyslipidemia 2018R JannahPas encore d'évaluation
- Nutrition and MSDocument62 pagesNutrition and MSzolhas2018Pas encore d'évaluation
- Effects of Oleic Acid: Review Article Doi: 10.17546/msd.25609Document8 pagesEffects of Oleic Acid: Review Article Doi: 10.17546/msd.25609Radwan AjoPas encore d'évaluation
- CVD and MNTDocument90 pagesCVD and MNTNadia AbbasPas encore d'évaluation
- Prediabetes HandoutDocument5 pagesPrediabetes HandoutAndra VantPas encore d'évaluation
- Effect of Walnut (Juglans Regia) Consumption On Hyperlipidemic AdultsDocument7 pagesEffect of Walnut (Juglans Regia) Consumption On Hyperlipidemic AdultsBETÜL KILINÇLIPas encore d'évaluation
- Human Nutrition and MetabolismDocument7 pagesHuman Nutrition and MetabolismMisyani MisyaniPas encore d'évaluation
- Effect of Low Carbohydrate High Fat Diet On LDL Cholesterol and Gene Expression in Normal Weight, Young Adults A Randomized Controlled StudyDocument10 pagesEffect of Low Carbohydrate High Fat Diet On LDL Cholesterol and Gene Expression in Normal Weight, Young Adults A Randomized Controlled StudyJennie ManobanPas encore d'évaluation
- Sindrom Metabolik Alwi ShahabDocument10 pagesSindrom Metabolik Alwi ShahabIndah Hime AzzahraPas encore d'évaluation
- Mini Case Study WeeblyDocument5 pagesMini Case Study Weeblyapi-270446591Pas encore d'évaluation
- Diabetes Case StudyDocument3 pagesDiabetes Case Studydsaitta108Pas encore d'évaluation
- Original Research ArticleDocument21 pagesOriginal Research ArticleRafaela SanchesPas encore d'évaluation
- Chapter 31 Dyslipidemia UpdatedDocument37 pagesChapter 31 Dyslipidemia UpdatedMai TarekPas encore d'évaluation
- 7.systematic Review and Meta-Analysis of Clinical Trials of The Effects of Low Carbohydrate Diets On Cardiovascular Risk Factors.Document19 pages7.systematic Review and Meta-Analysis of Clinical Trials of The Effects of Low Carbohydrate Diets On Cardiovascular Risk Factors.Ambar Sofía MieresPas encore d'évaluation
- 1 s2.0 S1056617119316009 MainDocument8 pages1 s2.0 S1056617119316009 Mainmekdes abebePas encore d'évaluation
- Bahan Semiloka LitbangDocument15 pagesBahan Semiloka LitbangArumrukmasariPas encore d'évaluation
- Fisiopatologia Sindrome MetabolicoDocument9 pagesFisiopatologia Sindrome MetabolicoEmilio MoncadaPas encore d'évaluation
- PBL Case 1 LODocument2 pagesPBL Case 1 LObryan chanPas encore d'évaluation
- Omega-3 Fatty Acids, Polymorphisms and Lipid Related Cardiovascular Disease Risk Factors in The Inuit PopulationDocument9 pagesOmega-3 Fatty Acids, Polymorphisms and Lipid Related Cardiovascular Disease Risk Factors in The Inuit Populationyoga diputraPas encore d'évaluation
- AtherosclerosisDocument29 pagesAtherosclerosisneeraj banaPas encore d'évaluation
- Cardiovasc.-Nutr Therapy - Univ PlkrayaDocument67 pagesCardiovasc.-Nutr Therapy - Univ PlkrayaFaridah Yuwono 28Pas encore d'évaluation
- DM - NotesDocument7 pagesDM - NotesAli salimPas encore d'évaluation
- Sindrom MetabolikDocument9 pagesSindrom MetabolikUlquiorra SchifferPas encore d'évaluation
- Olive Oil Fact Sheet 01Document2 pagesOlive Oil Fact Sheet 01vksk1951Pas encore d'évaluation
- Metabolik SindromeDocument46 pagesMetabolik SindromePAn Lover'zPas encore d'évaluation
- Chronic LeukemiaDocument12 pagesChronic LeukemiaJuan RamirezPas encore d'évaluation
- Massey University: Manawatu & Albany CampusesDocument4 pagesMassey University: Manawatu & Albany CampusesJuan RamirezPas encore d'évaluation
- Massey University: Manawatu & Albany CampusesDocument4 pagesMassey University: Manawatu & Albany CampusesJuan RamirezPas encore d'évaluation
- 2013Document17 pages2013Juan RamirezPas encore d'évaluation
- I4 I10 0901Document4 pagesI4 I10 0901Juan RamirezPas encore d'évaluation
- Massey University: Auckland CampusDocument2 pagesMassey University: Auckland CampusJuan RamirezPas encore d'évaluation
- 10ALB 196 207 Final ExamDocument4 pages10ALB 196 207 Final ExamJuan RamirezPas encore d'évaluation
- Koagulasie ( Vit K) : Naphthoquinone Ring Different Side ChainsDocument4 pagesKoagulasie ( Vit K) : Naphthoquinone Ring Different Side ChainsJuan RamirezPas encore d'évaluation
- Vegetarian DietsDocument7 pagesVegetarian DietsJuan RamirezPas encore d'évaluation
- Molecular Signatures of Natural Selection: Rasmus NielsenDocument24 pagesMolecular Signatures of Natural Selection: Rasmus NielsenJuan RamirezPas encore d'évaluation
- Fs Slim Cigarettes enDocument1 pageFs Slim Cigarettes enSurya MallaPas encore d'évaluation
- The Environment Protection Act - 1986Document9 pagesThe Environment Protection Act - 1986hitendrasentaPas encore d'évaluation
- Consolidated Nutritional Status Baseline 2018 2019Document12 pagesConsolidated Nutritional Status Baseline 2018 2019michael segundo0% (1)
- Lean and FabDocument13 pagesLean and Fabchucky_4000Pas encore d'évaluation
- Chapters1 5Document75 pagesChapters1 5api-3722454100% (2)
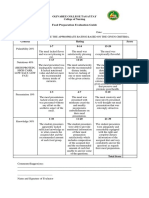
- Food Preparation Evaluation Guide: Olivarez College Tagaytay College of NursingDocument2 pagesFood Preparation Evaluation Guide: Olivarez College Tagaytay College of NursingRaquel M. MendozaPas encore d'évaluation
- Skala TidurDocument2 pagesSkala TidurMaris JessicaPas encore d'évaluation
- Argumentative Essay On Obesity PDFDocument2 pagesArgumentative Essay On Obesity PDFGertrude Yasha Anne RosalesPas encore d'évaluation
- Draft 1 Seminar 2 FitFoodsDocument200 pagesDraft 1 Seminar 2 FitFoodsTEDY TEDYPas encore d'évaluation
- Test Bank For Contemporary Nutrition 8th Edition Gordon WardlawDocument20 pagesTest Bank For Contemporary Nutrition 8th Edition Gordon WardlawJustin Zeches100% (31)
- What Is A Diet Window?: A Diet Based On A Nobel Prize Winning Idea Can Help You Lose Weight and Slow Down AgingDocument4 pagesWhat Is A Diet Window?: A Diet Based On A Nobel Prize Winning Idea Can Help You Lose Weight and Slow Down Agingcatalin_croitoruPas encore d'évaluation
- Exercise For Fitness: "Strengthen Your Faith Through Physical Exercise"Document19 pagesExercise For Fitness: "Strengthen Your Faith Through Physical Exercise"Goodness- Gabihan, IyannaPas encore d'évaluation
- 16 Strategies For Successful Fat LossDocument12 pages16 Strategies For Successful Fat LosstobyPas encore d'évaluation
- Physical Fitness PDFDocument10 pagesPhysical Fitness PDFDennis GuavisPas encore d'évaluation
- BMI For AgeDocument2 pagesBMI For AgeNeil AtanacioPas encore d'évaluation
- Fit Over 40 GuideDocument29 pagesFit Over 40 GuideAngelaPas encore d'évaluation
- Health Guid Ind Docts kuwaitHG3Document128 pagesHealth Guid Ind Docts kuwaitHG3Harish KumarPas encore d'évaluation
- Air Based Hazards PDFDocument17 pagesAir Based Hazards PDFRiyan SyedPas encore d'évaluation
- The Perspective On Healthy Food Choices by TheDocument7 pagesThe Perspective On Healthy Food Choices by TheAlexandrea Jhoy M. ArgayosoPas encore d'évaluation
- Iversen - Schoenfeld No Time To Lift - Designing Time-Efficient Training ProgramDocument17 pagesIversen - Schoenfeld No Time To Lift - Designing Time-Efficient Training Programbarna284Pas encore d'évaluation
- BiaDocument7 pagesBiaDian WijayantiPas encore d'évaluation
- Smoking Webquest AssignmentDocument4 pagesSmoking Webquest Assignmentapi-238194604Pas encore d'évaluation
- Why Unhealthy Food Taste So GoodDocument3 pagesWhy Unhealthy Food Taste So GoodJorge Gutierrez0% (1)
- The Truth About CrossfitDocument15 pagesThe Truth About CrossfitlionelxxlPas encore d'évaluation