Vous aimerez peut-être aussi
- Stroger Hospital Intern GuideDocument43 pagesStroger Hospital Intern Guidesgod34Pas encore d'évaluation
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionD'EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionPas encore d'évaluation
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionD'EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionPas encore d'évaluation
- Intern Ward Survival Guide 2009Document5 pagesIntern Ward Survival Guide 2009mediquest100% (1)
- Intern Survival Guide The UNC Department of MedicineDocument22 pagesIntern Survival Guide The UNC Department of MedicinecmirceaPas encore d'évaluation
- Internal Medicine Survival GuideDocument44 pagesInternal Medicine Survival GuideVSPas encore d'évaluation
- Utmck Survival Guide 2010Document46 pagesUtmck Survival Guide 2010sha89Pas encore d'évaluation
- Tsra Intern Survival Guide 9 12Document44 pagesTsra Intern Survival Guide 9 12johntheuglyllamaPas encore d'évaluation
- Intern Survival Guide (UIC)Document51 pagesIntern Survival Guide (UIC)medstick100% (1)
- Common Medical NotationsDocument3 pagesCommon Medical NotationssaltarisPas encore d'évaluation
- Intern Ward SuccessDocument3 pagesIntern Ward Successporfyra_Pas encore d'évaluation
- Common Calls For InternsDocument1 pageCommon Calls For Internstheusuals100% (1)
- Intern Survival GuideDocument12 pagesIntern Survival GuideHunter RossPas encore d'évaluation
- Appendix and Acknowledgements SummaryDocument58 pagesAppendix and Acknowledgements Summaryniharjhatn100% (1)
- Intern Survival Guide 2014-2015Document145 pagesIntern Survival Guide 2014-2015PreaisPas encore d'évaluation
- Neurology For Family MedicineDocument21 pagesNeurology For Family MedicineSayeed Khan100% (1)
- ClinicalSurvivalGuide 2012 2013Document62 pagesClinicalSurvivalGuide 2012 2013Zebram Zee100% (1)
- Usmle Step 2 CsDocument70 pagesUsmle Step 2 CsAlvi MuldaniPas encore d'évaluation
- UPenn Clinic GuideDocument114 pagesUPenn Clinic GuideVeronica AlexanderPas encore d'évaluation
- UCSF Hospitalist Handbook 2002Document236 pagesUCSF Hospitalist Handbook 2002wjdittmar50% (2)
- Ob GynDocument4 pagesOb GynAstariAnnemariePas encore d'évaluation
- Cardiac Arrest VF/Pulseless VT Learning Station ChecklistDocument5 pagesCardiac Arrest VF/Pulseless VT Learning Station ChecklistMaryam FadahPas encore d'évaluation
- 11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17Document13 pages11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17M100% (1)
- Docslide - Us Family Medicine Shelf Reviewpptx Read OnlyDocument142 pagesDocslide - Us Family Medicine Shelf Reviewpptx Read OnlyDavid DengPas encore d'évaluation
- 2017-2018 Intern GuideDocument31 pages2017-2018 Intern GuideaskjagPas encore d'évaluation
- The Unofficial Clinical Clerkship Survival Guide: LouisvilleDocument65 pagesThe Unofficial Clinical Clerkship Survival Guide: LouisvilleAffan HaqPas encore d'évaluation
- Intern Survival Guide 2012-2013Document23 pagesIntern Survival Guide 2012-2013alaa100% (1)
- Preventative Care and Common ConditionsDocument44 pagesPreventative Care and Common ConditionsJoshuaPas encore d'évaluation
- The Book About MCQDocument2 pagesThe Book About MCQchien_truongPas encore d'évaluation
- Ideal Inpatient Progress Notes Template of Ideal Progress NoteDocument2 pagesIdeal Inpatient Progress Notes Template of Ideal Progress Notebrianzfl100% (1)
- Antibiotic Prescribing in Primary Care - Therapeutic Guidelines Summary Table 2019Document2 pagesAntibiotic Prescribing in Primary Care - Therapeutic Guidelines Summary Table 2019RL100% (1)
- Internal Med TipsDocument2 pagesInternal Med TipsNick100% (1)
- Housestaff Survival GuideDocument107 pagesHousestaff Survival GuideJamal Ansari100% (1)
- Efast: Name Position Normal US Pic Abnormal US Pic SubcostalDocument4 pagesEfast: Name Position Normal US Pic Abnormal US Pic SubcostalMaryam FadahPas encore d'évaluation
- Intern Survival Guide: DisclaimerDocument23 pagesIntern Survival Guide: DisclaimerKing David100% (1)
- How To Study For Third Year RotationsDocument5 pagesHow To Study For Third Year RotationsAudia IndrianPas encore d'évaluation
- Intern Survival Guide Ward 2Document44 pagesIntern Survival Guide Ward 2Keith Swait Zin50% (2)
- Word AssociationDocument27 pagesWord AssociationMilan Kolovrat100% (1)
- Family Practice Handbook 4edDocument593 pagesFamily Practice Handbook 4eddeb haart100% (1)
- Clinical Pearls in General Internal Medicine 2012 (Mayo Clinic)Document7 pagesClinical Pearls in General Internal Medicine 2012 (Mayo Clinic)PkernPas encore d'évaluation
- Sources: CardiovascularDocument117 pagesSources: CardiovascularMohannad AlfadhalPas encore d'évaluation
- Internal Medicine EOR-PrintDocument276 pagesInternal Medicine EOR-PrintDanielle GroupfivePas encore d'évaluation
- Peds EORDocument17 pagesPeds EORRachel BarrosPas encore d'évaluation
- Family Medicine NotesDocument52 pagesFamily Medicine NotesGene Paolo Janzi SaplaPas encore d'évaluation
- COMLEX Level 2 PE Case DifferentialsDocument8 pagesCOMLEX Level 2 PE Case DifferentialsBenny Wu100% (1)
- Internal Medicine NotesDocument54 pagesInternal Medicine NotesKiara Govender100% (1)
- EM Basic - Pocket GuideDocument97 pagesEM Basic - Pocket Guidemainertoo100% (2)
- Third Year Survival GuideDocument25 pagesThird Year Survival GuideManish KPas encore d'évaluation
- Board Certified Nurse Practitioner in Savannah GA Resume Michele StephensDocument4 pagesBoard Certified Nurse Practitioner in Savannah GA Resume Michele StephensMicheleStephens100% (1)
- Rosh ReviewsDocument19 pagesRosh ReviewsTracy NwannePas encore d'évaluation
- Sports MedicineDocument32 pagesSports Medicinersimranjit100% (1)
- 2008 It e CritiqueDocument78 pages2008 It e Critiquerofi modiPas encore d'évaluation
- Internal MedicineDocument138 pagesInternal MedicineMohammed S. Al GhamdiPas encore d'évaluation
- Clinical Clerkship Survival Guide: USF Morsani College of Medicine Class of 2020Document56 pagesClinical Clerkship Survival Guide: USF Morsani College of Medicine Class of 2020Lawangeenz40% (5)
- Success On The Wards 2008-09Document70 pagesSuccess On The Wards 2008-09learss79Pas encore d'évaluation
- The 10-Minute Physical Exam: recognizing medical syndromesD'EverandThe 10-Minute Physical Exam: recognizing medical syndromesPas encore d'évaluation
- Citrate CRRT Anticoagulation ProtocolDocument5 pagesCitrate CRRT Anticoagulation ProtocolXavi AnpiPas encore d'évaluation
- Chapter 20 - Postoperative Nursing ManagementDocument17 pagesChapter 20 - Postoperative Nursing ManagementTeemara KingPas encore d'évaluation
- Antibiotic Guidelines (2020) - 0Document55 pagesAntibiotic Guidelines (2020) - 0yudhit bessiePas encore d'évaluation
- Transfusion Medicine Thesis TopicsDocument4 pagesTransfusion Medicine Thesis Topicsgjggsf72100% (2)
- Meningitis PDFDocument10 pagesMeningitis PDFAlfatahadi SPas encore d'évaluation
- Acute Kidney Injury: Authors: Alistair ConnellDocument5 pagesAcute Kidney Injury: Authors: Alistair ConnellRobertPas encore d'évaluation
- Efficacy and Safety of A Paired Sedation and Ventilator Weaning Prtocol For Mechanically Ventilated Patients in Intesive Care ABC)Document16 pagesEfficacy and Safety of A Paired Sedation and Ventilator Weaning Prtocol For Mechanically Ventilated Patients in Intesive Care ABC)Miguel CachonPas encore d'évaluation
- Aki 6Document12 pagesAki 6WindaPas encore d'évaluation
- IDSA Guideline PDFDocument80 pagesIDSA Guideline PDFArifHidayatPas encore d'évaluation
- Complicatii PneumonieDocument9 pagesComplicatii PneumonieTatiana JalbaPas encore d'évaluation
- Critical Care Nursing ClinicsDocument133 pagesCritical Care Nursing ClinicsJune DumdumayaPas encore d'évaluation
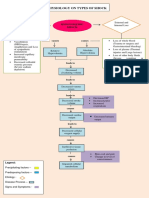
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaPas encore d'évaluation
- DR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFDocument38 pagesDR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFNONAPas encore d'évaluation
- Hemodynamic response to β-blockers in severe sepsis and septic shock: A review of current literatureDocument6 pagesHemodynamic response to β-blockers in severe sepsis and septic shock: A review of current literatureIris AszalosPas encore d'évaluation
- ACF JD Plastic Surgery Birmingham 2023Document3 pagesACF JD Plastic Surgery Birmingham 2023Oscar Zhen Yu WongPas encore d'évaluation
- United Republic of Tanzania: Ministry of Health, Community Development, Gender, Elderly and ChildrenDocument50 pagesUnited Republic of Tanzania: Ministry of Health, Community Development, Gender, Elderly and ChildrenHAMIS MASOUDPas encore d'évaluation
- Damage Control Management y Polytrauma PatientDocument324 pagesDamage Control Management y Polytrauma PatientMauri ParadedaPas encore d'évaluation
- 2023 - Hydrocortisone in Severe CommunityDocument11 pages2023 - Hydrocortisone in Severe CommunitygiseladlrPas encore d'évaluation
- Variability in The Hemodynamic Response To Fluid Bolus in Pediatric Septic Shock - 1Document11 pagesVariability in The Hemodynamic Response To Fluid Bolus in Pediatric Septic Shock - 1diflopasPas encore d'évaluation
- SIRS and AAA 05-04-04Document12 pagesSIRS and AAA 05-04-04Gargi MishraPas encore d'évaluation
- DrNB CRITICAL CARE MEDICINE Paper3Document4 pagesDrNB CRITICAL CARE MEDICINE Paper3aparnapingali0Pas encore d'évaluation
- Multi OrganDocument10 pagesMulti OrganthyinkslingerPas encore d'évaluation
- Management Sepsis TerkiniDocument82 pagesManagement Sepsis TerkiniSyahrul HamidPas encore d'évaluation
- Jan2016 Mackie Research - Spectral MedicalDocument33 pagesJan2016 Mackie Research - Spectral MedicalAnonymous sXJ5jvoPas encore d'évaluation
- Multi Organ Dysfunction SyndromeDocument40 pagesMulti Organ Dysfunction SyndromeDr. Jayesh PatidarPas encore d'évaluation
- Oral Station ScenarioDocument3 pagesOral Station ScenariojrworthingtonPas encore d'évaluation
- EMRAP: Emergency Medicine Reviews and PerspectivesDocument3 pagesEMRAP: Emergency Medicine Reviews and PerspectivesAshleyPas encore d'évaluation
- Fluid Therapy and ShockDocument8 pagesFluid Therapy and ShockJuan Francisco SánchezPas encore d'évaluation
- 3 - Sepsis Blood Culture Ss 20180505 DwsDocument26 pages3 - Sepsis Blood Culture Ss 20180505 DwsselaturPas encore d'évaluation
- ThrombocytopeniaDocument12 pagesThrombocytopeniatantyPas encore d'évaluation