Vous aimerez peut-être aussi
- CBLM CaregivingDocument116 pagesCBLM CaregivingGreyz Blas83% (6)
- New Frontiers SB 1Document8 pagesNew Frontiers SB 1SD CIS KOTA CIREBON JAWA BARATPas encore d'évaluation
- Jurnal Internasional Korea DMDocument9 pagesJurnal Internasional Korea DMzahradeswitamuftiPas encore d'évaluation
- 2010-High-Sensitivoty of C-Reactive Protein and CancerDocument8 pages2010-High-Sensitivoty of C-Reactive Protein and CancerThalia KarampasiPas encore d'évaluation
- Jurnal 6Document8 pagesJurnal 6OziPas encore d'évaluation
- Relationship Between C-Reactive Protein, White Blood Cell Count and Metabolic Syndrome in Nigerians With Type 2 Diabetes MellitusDocument11 pagesRelationship Between C-Reactive Protein, White Blood Cell Count and Metabolic Syndrome in Nigerians With Type 2 Diabetes MellitusPaul Gesswein FonatabaPas encore d'évaluation
- Paper Insulin Resistance and Ferritin As Major Determinants of Nonalcoholic Fatty Liver Disease in Apparently Healthy Obese PatientsDocument7 pagesPaper Insulin Resistance and Ferritin As Major Determinants of Nonalcoholic Fatty Liver Disease in Apparently Healthy Obese PatientsNike Dwi Putri LestariPas encore d'évaluation
- Generating A Reference Interval For Fasting Serum Insulin in Healthy Nondiabetic Adult Chinese MenDocument5 pagesGenerating A Reference Interval For Fasting Serum Insulin in Healthy Nondiabetic Adult Chinese MenTanveerPas encore d'évaluation
- Do Proton Pump Inhibitors Increase Mortality in Cirrhotic Patients With Spontaneous Bacterial Peritonitis?Document29 pagesDo Proton Pump Inhibitors Increase Mortality in Cirrhotic Patients With Spontaneous Bacterial Peritonitis?Muhammad Rehan AnisPas encore d'évaluation
- Expression of Renal Injury Markers Among Diabetic Patients in The University of Port Harcourt Teaching HospitalDocument8 pagesExpression of Renal Injury Markers Among Diabetic Patients in The University of Port Harcourt Teaching Hospitalijmb333Pas encore d'évaluation
- Nutrients: Nutritional Adequacy and Latent Tuberculosis Infection in End-Stage Renal Disease PatientsDocument8 pagesNutrients: Nutritional Adequacy and Latent Tuberculosis Infection in End-Stage Renal Disease PatientsMarwa AmrangPas encore d'évaluation
- Met 2019 0059Document6 pagesMet 2019 0059raihannah othmanPas encore d'évaluation
- Diabetes1 KoreaDocument10 pagesDiabetes1 KoreaJimmyPas encore d'évaluation
- 1 s2.0 S1051227620302909 MainDocument8 pages1 s2.0 S1051227620302909 MainIván OsunaPas encore d'évaluation
- Association Between Serum Cystatin C and Diabetic Peripheral Neuropathy: A Cross-Sectional Study of A Chinese Type 2 Diabetic PopulationDocument8 pagesAssociation Between Serum Cystatin C and Diabetic Peripheral Neuropathy: A Cross-Sectional Study of A Chinese Type 2 Diabetic PopulationSakdeep SinghPas encore d'évaluation
- Tight GlycemicDocument10 pagesTight GlycemicIsmail Mohammed AbdelgawadPas encore d'évaluation
- Serum Albumin Level Adjusted With C-Reactive Protein Predicts Hemodialysis Patient SurvivalDocument9 pagesSerum Albumin Level Adjusted With C-Reactive Protein Predicts Hemodialysis Patient Survivalmelda lestari haidirPas encore d'évaluation
- Metabolic Cardiovascular Disease Risk Factors and Their Clustering in Subclinical HypothyroidismDocument7 pagesMetabolic Cardiovascular Disease Risk Factors and Their Clustering in Subclinical HypothyroidismMaria Alice BourneufPas encore d'évaluation
- Study of Lipid Profile in Coronary Heart Disease Patients in LibyaDocument9 pagesStudy of Lipid Profile in Coronary Heart Disease Patients in LibyaInternational Medical PublisherPas encore d'évaluation
- Phagocytic Activity Is Impaired in Type 2 Diabetes Mellitus and Increases After Metabolic ImprovementDocument6 pagesPhagocytic Activity Is Impaired in Type 2 Diabetes Mellitus and Increases After Metabolic ImprovementJenny JennyssimaPas encore d'évaluation
- Jurnal Bu Sulis 1Document6 pagesJurnal Bu Sulis 1PitoAdhiPas encore d'évaluation
- Effect of BmiDocument5 pagesEffect of BmiSyaiful Putra RanaPas encore d'évaluation
- The Metabolic Syndrome: Comparison of Newly Proposed IDF, Modified ATP III and WHO Criteria and Their AgreementsDocument6 pagesThe Metabolic Syndrome: Comparison of Newly Proposed IDF, Modified ATP III and WHO Criteria and Their AgreementsjoelPas encore d'évaluation
- 1 s2.0 S1051227616301789 MainDocument7 pages1 s2.0 S1051227616301789 MainResearch OfficePas encore d'évaluation
- Impact of A Nurse Short Message Service Intervention For Patients With DiabetesDocument6 pagesImpact of A Nurse Short Message Service Intervention For Patients With DiabetesFatima Akbar.Pas encore d'évaluation
- s10554 014 0541 6Document11 pagess10554 014 0541 6Wami FadelPas encore d'évaluation
- The Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsDocument11 pagesThe Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsThinh VinhPas encore d'évaluation
- Habitual Coffee Intake, Genetic Polymorphisms, and Type 2 DiabetesDocument8 pagesHabitual Coffee Intake, Genetic Polymorphisms, and Type 2 DiabetesRengganis PutriPas encore d'évaluation
- Active Smoking, Passive Smoking, and Risk of Nonalcoholic Fatty Liver Disease (NAFLD) : A Population-Based Study in ChinaDocument7 pagesActive Smoking, Passive Smoking, and Risk of Nonalcoholic Fatty Liver Disease (NAFLD) : A Population-Based Study in ChinaYelvi Novita RozaPas encore d'évaluation
- Jurnal DWIDocument6 pagesJurnal DWIDwi Asti Lestari PandePas encore d'évaluation
- Manuscript Category: Original Article: DR. YUYA ITANO (Orcid ID: 0000-0001-5287-8550)Document25 pagesManuscript Category: Original Article: DR. YUYA ITANO (Orcid ID: 0000-0001-5287-8550)MarcelliaPas encore d'évaluation
- Chemistry - Ijapbcr - Study of C-Reactive Protein and - Mohd ShakeelDocument6 pagesChemistry - Ijapbcr - Study of C-Reactive Protein and - Mohd ShakeelTJPRC PublicationsPas encore d'évaluation
- Prevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionDocument10 pagesPrevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionZaskia PutriPas encore d'évaluation
- Nutrients 12 00878Document13 pagesNutrients 12 00878Ardian AshadiPas encore d'évaluation
- Serum Taurine and Risk of Coronary Heart Disease: A Prospective, Nested Case-Control StudyDocument10 pagesSerum Taurine and Risk of Coronary Heart Disease: A Prospective, Nested Case-Control StudyThalia KarampasiPas encore d'évaluation
- CIA 58682 Prognostic Value of Severity Indicators of Nursing Home Acqu 021114Document8 pagesCIA 58682 Prognostic Value of Severity Indicators of Nursing Home Acqu 021114Andres Ramos CardozoPas encore d'évaluation
- Journal Stress OksidatifDocument8 pagesJournal Stress OksidatifMiftakhur RohmahPas encore d'évaluation
- Test Thesis 2 10Document36 pagesTest Thesis 2 10adam yassinePas encore d'évaluation
- Management of Lifestyle Factors in Individuals With Cirrhosis: A Pragmatic ReviewDocument9 pagesManagement of Lifestyle Factors in Individuals With Cirrhosis: A Pragmatic ReviewsavitageraPas encore d'évaluation
- Dietary Protein Intake, Protein Energy Wasting - NUTRIENTS 2019Document12 pagesDietary Protein Intake, Protein Energy Wasting - NUTRIENTS 2019Marilu VillalobosPas encore d'évaluation
- Jurnal Kimia 8Document13 pagesJurnal Kimia 8Rizka Nurul FirdausPas encore d'évaluation
- Worldwide Trends in Diabetes Since 1980Document484 pagesWorldwide Trends in Diabetes Since 1980L P Lozada MartinezPas encore d'évaluation
- 1 s2.0 S1051227619300020 MainDocument9 pages1 s2.0 S1051227619300020 MainRomário de Macedo EspíndolaPas encore d'évaluation
- Using The EQ-5D Index Score As A Predictor of Outcomes in Patients With Type 2 Diabetes - Clarke May08Document20 pagesUsing The EQ-5D Index Score As A Predictor of Outcomes in Patients With Type 2 Diabetes - Clarke May08Haneesha MuddasaniPas encore d'évaluation
- 7decaf9c Cb18 4623 Bced Ecef2197e451Document25 pages7decaf9c Cb18 4623 Bced Ecef2197e451PrabhuPas encore d'évaluation
- 1471 2369 14 191 PDFDocument9 pages1471 2369 14 191 PDFhanifahrafaPas encore d'évaluation
- Association Between SocioeconomicDocument10 pagesAssociation Between SocioeconomicEduardo JohannesPas encore d'évaluation
- Thesis On Liver DiseaseDocument5 pagesThesis On Liver DiseaseCustomNotePaperCanada100% (1)
- Research Paper On Liver DiseaseDocument5 pagesResearch Paper On Liver Diseaseefjem40q100% (1)
- Nutrients: Micronutrient Status in 153 Patients With Anorexia NervosaDocument10 pagesNutrients: Micronutrient Status in 153 Patients With Anorexia NervosaReza Yusna HanastaPas encore d'évaluation
- Excess Protein Intake Relative To Fiber and Cardiovascular Events in Elderly Men With Chronic Kidney DiseaseDocument6 pagesExcess Protein Intake Relative To Fiber and Cardiovascular Events in Elderly Men With Chronic Kidney Diseaseluis Gomez VallejoPas encore d'évaluation
- 1nnnnn ... A Qbqn2i29191s D..... Snsjwnwbs SSWQJQKQ 1111111 60-167Document8 pages1nnnnn ... A Qbqn2i29191s D..... Snsjwnwbs SSWQJQKQ 1111111 60-167Red DiggerPas encore d'évaluation
- Assessment of Creactive Protein Lpid Profile and Body Mass Index in Type2 Diabetes Mellitus in Sudanese PatientsDocument9 pagesAssessment of Creactive Protein Lpid Profile and Body Mass Index in Type2 Diabetes Mellitus in Sudanese PatientsMotasem Sirag Mohmmed othmanPas encore d'évaluation
- Anti-Inflammatory Effects of ExerciseDocument10 pagesAnti-Inflammatory Effects of Exercisejbone918Pas encore d'évaluation
- Effect of Zinc Supplementation On Insulin Resistance and Metabolic Risk Factors in Obese Korean WomenDocument5 pagesEffect of Zinc Supplementation On Insulin Resistance and Metabolic Risk Factors in Obese Korean WomenFahmy2015Pas encore d'évaluation
- Baca IniDocument9 pagesBaca IniRahmi Annisa MaharaniPas encore d'évaluation
- Clinical PharmacyDocument6 pagesClinical PharmacyIrene KristiantiPas encore d'évaluation
- Analysis of Blood Glucose Distribution Characteristics and Its Risk Factors Among A Health Examination Population in Wuhu (China)Document9 pagesAnalysis of Blood Glucose Distribution Characteristics and Its Risk Factors Among A Health Examination Population in Wuhu (China)Aleksa CopicPas encore d'évaluation
- Higher Selenium Status Is Associated With Adverse Blood Lipid Profile in British AdultsDocument7 pagesHigher Selenium Status Is Associated With Adverse Blood Lipid Profile in British AdultsHerly Maulida SurdhawatiPas encore d'évaluation
- The Effects of Lead Exposure On Serum Uric Acid and Hyperuricemia in Chinese Adults: A Cross-Sectional StudyDocument11 pagesThe Effects of Lead Exposure On Serum Uric Acid and Hyperuricemia in Chinese Adults: A Cross-Sectional StudyriaPas encore d'évaluation
- Complementary and Alternative Medical Lab Testing Part 8: UrologyD'EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyÉvaluation : 3 sur 5 étoiles3/5 (1)
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderD'EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderPas encore d'évaluation
- Grade 9 DLP Week 1 Day1 2Document11 pagesGrade 9 DLP Week 1 Day1 2Rando Estañero MonsaludPas encore d'évaluation
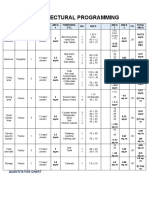
- Architectural Programming: Quantitative ChartDocument3 pagesArchitectural Programming: Quantitative Chartmiriam martinez50% (2)
- Goldenville School of Montessori, Inc.: Matimbubong, San Ildefonso, BulacanDocument4 pagesGoldenville School of Montessori, Inc.: Matimbubong, San Ildefonso, BulacanKenneth Delos SantosPas encore d'évaluation
- Recette World Chocolate Masters - InfiniteDocument1 pageRecette World Chocolate Masters - InfiniteTarak ZayaniPas encore d'évaluation
- Care Sheet - Bearded DragonDocument4 pagesCare Sheet - Bearded DragonJohn Gamesby100% (1)
- Mobile - Hyderabadi Chicken Biryani Recipe, HyderabadiDocument2 pagesMobile - Hyderabadi Chicken Biryani Recipe, HyderabadiBarath GunasekaranPas encore d'évaluation
- Cephaleuros VirescensDocument6 pagesCephaleuros VirescensAlexis Romero DobbertinPas encore d'évaluation
- Sex Tour Part DeuxDocument1 pageSex Tour Part DeuxAvel ManansalaPas encore d'évaluation
- Last Mile 5category LayoutsDocument24 pagesLast Mile 5category LayoutsManoj NakraPas encore d'évaluation
- Notes Form 2 Chapter 4Document4 pagesNotes Form 2 Chapter 4lembu_sihat7783% (6)
- S in Hort Te Ntroduc Est Ans Tion Un Wer Ke Nit, Test Eys A t1Document6 pagesS in Hort Te Ntroduc Est Ans Tion Un Wer Ke Nit, Test Eys A t1Teachers SMG eduPas encore d'évaluation
- TítDocument14 pagesTítAnhTuyet ThieuPas encore d'évaluation
- A Warm Wedding and A New Bride of Young Master LuDocument48 pagesA Warm Wedding and A New Bride of Young Master LuANNA ANETA50% (2)
- d.3. Blue Dairy Corp Vs NLRC, G.R. No. 129843, September 14, 1999Document5 pagesd.3. Blue Dairy Corp Vs NLRC, G.R. No. 129843, September 14, 1999LawrenceAltezaPas encore d'évaluation
- Shawarma Spice Blend Recipe - Minimalist Baker RecipesDocument9 pagesShawarma Spice Blend Recipe - Minimalist Baker RecipesDenis JPas encore d'évaluation
- 6 291 1477120320241 244Document4 pages6 291 1477120320241 244DarshanPas encore d'évaluation
- ISKCON Desire Tree - Vanilla Butter CakeDocument2 pagesISKCON Desire Tree - Vanilla Butter CakeISKCON desire treePas encore d'évaluation
- Student Name:: Welcome To "Introduction To ISO 22000 Food Safety Management Systems"Document15 pagesStudent Name:: Welcome To "Introduction To ISO 22000 Food Safety Management Systems"frawatPas encore d'évaluation
- Patapon 2Document59 pagesPatapon 2Dennis LubianoPas encore d'évaluation
- The Gmo in Our FoodDocument23 pagesThe Gmo in Our FoodHaiz MainePas encore d'évaluation
- Rana PackagingDocument26 pagesRana PackagingVignesh DurairajPas encore d'évaluation
- Mat Leave LetterDocument11 pagesMat Leave LetterLeshlie OrdonioPas encore d'évaluation
- 101 Essential Tips Dog Care - 2015 PDFDocument74 pages101 Essential Tips Dog Care - 2015 PDFalavanisPas encore d'évaluation
- Thesis About Pandan LeavesDocument5 pagesThesis About Pandan Leavesmelissajacksonminneapolis100% (2)
- Report of Ashapura Volclay LTDDocument33 pagesReport of Ashapura Volclay LTDNiraj Patel100% (2)
- CHAPTER 1 Investegatory ReasearchDocument3 pagesCHAPTER 1 Investegatory ReasearchAngelica Alican Cerbito50% (2)
- Graham Elizabeth Devil On Horseback PDFDocument191 pagesGraham Elizabeth Devil On Horseback PDFMaheran Aljufri81% (27)
- UNIT 12" It Really WorksDocument2 pagesUNIT 12" It Really WorksZulfa raniPas encore d'évaluation