Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Berat Badan Lahir Rendah (BBLR) Di Kabupaten KudusDocument10 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Berat Badan Lahir Rendah (BBLR) Di Kabupaten KudusDellaPas encore d'évaluation
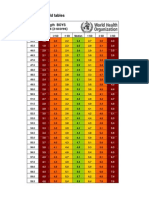
- Boys weight-length z-scores birth to 2 yearsDocument5 pagesBoys weight-length z-scores birth to 2 yearsAgus WijataPas encore d'évaluation
- Link Zoom KONIKA 18-19 OctDocument6 pagesLink Zoom KONIKA 18-19 OctAgus WijataPas encore d'évaluation
- 7869 40826 3 PB PDFDocument8 pages7869 40826 3 PB PDFHendra AjaPas encore d'évaluation
- Espr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedDocument1 pageEspr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedAgus WijataPas encore d'évaluation
- Wed SongDocument1 pageWed SongAgus WijataPas encore d'évaluation
- Pediatric Infectious Diseases Conference Focuses on COVID ManagementDocument2 pagesPediatric Infectious Diseases Conference Focuses on COVID ManagementAgus WijataPas encore d'évaluation
- 7869 40826 3 PB PDFDocument8 pages7869 40826 3 PB PDFHendra AjaPas encore d'évaluation
- Drug Doses 2017Document127 pagesDrug Doses 2017Yuliawati HarunaPas encore d'évaluation
- Pone 0026881Document5 pagesPone 0026881Agus WijataPas encore d'évaluation
- Pediatric Infectious Diseases Conference Focuses on COVID ManagementDocument2 pagesPediatric Infectious Diseases Conference Focuses on COVID ManagementAgus WijataPas encore d'évaluation
- Early Biochemical Indicators of Hypoxic-Ischemic Encephalopathy After Birth AsphyxiaDocument5 pagesEarly Biochemical Indicators of Hypoxic-Ischemic Encephalopathy After Birth AsphyxiaAgus WijataPas encore d'évaluation
- Pediatric Infectious Diseases Conference Focuses on COVID ManagementDocument2 pagesPediatric Infectious Diseases Conference Focuses on COVID ManagementAgus WijataPas encore d'évaluation
- Kids Games Powerpoint TemplateDocument26 pagesKids Games Powerpoint TemplateAgus WijataPas encore d'évaluation
- Mile-Stones of Develovment of ChildrenDocument9 pagesMile-Stones of Develovment of ChildrenAgus WijataPas encore d'évaluation
- Nna en November09Document3 pagesNna en November09Agus WijataPas encore d'évaluation
- CC 100Document4 pagesCC 100Agus WijataPas encore d'évaluation
- Biochemical Marker As Predictor of Outcome in Perinatal AsphyxiaDocument4 pagesBiochemical Marker As Predictor of Outcome in Perinatal AsphyxiaAgus WijataPas encore d'évaluation
- Edwin Kim, MD A. Wesley Burks, MD Michael Pistiner, MD, MMSCDocument1 pageEdwin Kim, MD A. Wesley Burks, MD Michael Pistiner, MD, MMSCAgus WijataPas encore d'évaluation
- a732b273a10a012b40c8154c371e732bDocument1 pagea732b273a10a012b40c8154c371e732bAgus WijataPas encore d'évaluation
- Status of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaDocument4 pagesStatus of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaAgus WijataPas encore d'évaluation
- 0 C 96053 C 581 B 042832000000Document1 page0 C 96053 C 581 B 042832000000Agus WijataPas encore d'évaluation
- Test Definition: NSE: Reporting Title: Neuron Specific Enolase, SDocument1 pageTest Definition: NSE: Reporting Title: Neuron Specific Enolase, SAgus WijataPas encore d'évaluation
- 5211Document7 pages5211Agus WijataPas encore d'évaluation
- SDQ Score Sheet and Instructions For Self ReoprtDocument2 pagesSDQ Score Sheet and Instructions For Self ReoprtAgus WijataPas encore d'évaluation
- Neuron-Specific Enolase As A Marker of The Severity and Outcome of Hypoxic Ischemic EncephalopathyDocument5 pagesNeuron-Specific Enolase As A Marker of The Severity and Outcome of Hypoxic Ischemic EncephalopathyAgus WijataPas encore d'évaluation
- SDQ Score Sheet and Instructions For Self ReoprtDocument2 pagesSDQ Score Sheet and Instructions For Self ReoprtAgus WijataPas encore d'évaluation
- 0 C 96053 C 581 B 042832000000Document1 page0 C 96053 C 581 B 042832000000Agus WijataPas encore d'évaluation
- Apnea NewbornDocument2 pagesApnea NewbornAgus WijataPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Congenital LaryngomalaciaDocument8 pagesCongenital LaryngomalaciaRettha SigiroPas encore d'évaluation
- عقد خدمDocument2 pagesعقد خدمtasheelonlinePas encore d'évaluation
- Manu SkripDocument20 pagesManu SkripzanimarPas encore d'évaluation
- Brett Stolberg 100112479 - ResumeDocument1 pageBrett Stolberg 100112479 - Resumeapi-193834982Pas encore d'évaluation
- Sustainability ReportDocument84 pagesSustainability ReportBhavan YadavPas encore d'évaluation
- Cardiovascular NotesDocument18 pagesCardiovascular NotesCathy SantosPas encore d'évaluation
- OPD Network ListDocument354 pagesOPD Network ListSHAIKH ABDUL AZIZ salim bashaPas encore d'évaluation
- Central Adult and Pediatric in Tensive Care UnitDocument4 pagesCentral Adult and Pediatric in Tensive Care UnitChris T NaPas encore d'évaluation
- Reiki Tummo Brochure 2013Document2 pagesReiki Tummo Brochure 2013Alicia TerryPas encore d'évaluation
- Being A Medical DoctorDocument14 pagesBeing A Medical DoctorMichael Bill GihonPas encore d'évaluation
- Pneumonia Care PlanDocument1 pagePneumonia Care Plantcumurphish67% (3)
- Heart Failure Lily ModifiedDocument57 pagesHeart Failure Lily ModifiedSabila FatimahPas encore d'évaluation
- How To Make An ELearning ModuleDocument22 pagesHow To Make An ELearning ModulePradeep RawatPas encore d'évaluation
- Maintenance Scheduling For Electrical EquipmentDocument82 pagesMaintenance Scheduling For Electrical Equipmentduonza100% (6)
- Pharmaceutical Microbiology Conference 2011 - SMi GroupDocument3 pagesPharmaceutical Microbiology Conference 2011 - SMi GroupTim SandlePas encore d'évaluation
- Syringe CompatibilityDocument1 pageSyringe CompatibilityRaju NiraulaPas encore d'évaluation
- S. No Name and Address Form 25 Dated Validupto Form 28 Dated Validupto 1 List of Pharmaceuticals Manufacturing CompaniesDocument52 pagesS. No Name and Address Form 25 Dated Validupto Form 28 Dated Validupto 1 List of Pharmaceuticals Manufacturing CompaniesSimon YiuPas encore d'évaluation
- Full Plate Diet BookDocument164 pagesFull Plate Diet BookScarlettNyx100% (4)
- The NBCP Referral Code SubDocument4 pagesThe NBCP Referral Code SubArcon Solite BarbanidaPas encore d'évaluation
- Assessed Conference Presentations ScheduleDocument2 pagesAssessed Conference Presentations ScheduleAna Maria Uribe AguirrePas encore d'évaluation
- Talisay Leaf Extract Cures Betta Fish in Less Time than Methylene BlueDocument8 pagesTalisay Leaf Extract Cures Betta Fish in Less Time than Methylene BlueMuhammad Rehan Said100% (1)
- Voyeuristic Disorder SymptomsDocument7 pagesVoyeuristic Disorder SymptomsgoyaPas encore d'évaluation
- IWA Publishing - Anaerobic Reactors For Sewage Treatment - Design, Construction and Operation - 2020-01-10Document1 pageIWA Publishing - Anaerobic Reactors For Sewage Treatment - Design, Construction and Operation - 2020-01-10JOHNY ALEJANDRO GARCIA SEPULVEDAPas encore d'évaluation
- Yoga Your Home Practice CompanionDocument257 pagesYoga Your Home Practice Companionjohncoltrane97% (33)
- TULUA Lipoabdominoplasty Transversal Aponeurotic.12Document14 pagesTULUA Lipoabdominoplasty Transversal Aponeurotic.12Carolina Ormaza Giraldo100% (1)
- Week 4-Physical Fitness TestDocument38 pagesWeek 4-Physical Fitness TestCatherine Sagario OliquinoPas encore d'évaluation
- NCP Gastric CancerDocument7 pagesNCP Gastric CancerAnonymous XvwKtnSrMR100% (4)
- Covidsafe Application Privacy Impact AssessmentDocument78 pagesCovidsafe Application Privacy Impact AssessmentMichael Smith100% (1)
- IFUk en 310250 07 PDFDocument14 pagesIFUk en 310250 07 PDFKhaled AlkhawaldehPas encore d'évaluation
- Complaints Handling: BDA AdviceDocument8 pagesComplaints Handling: BDA Advicedruzair007Pas encore d'évaluation