Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Concurrent TreatmentDocument257 pagesConcurrent TreatmentHector Arenas100% (3)
- Long Term Effects of Parental Alienation On Adult Children by Dr. Amy J.L. BakerDocument15 pagesLong Term Effects of Parental Alienation On Adult Children by Dr. Amy J.L. BakerTalia Schwartz100% (2)
- Absen Harian Coass BedahDocument1 pageAbsen Harian Coass BedahasddfggPas encore d'évaluation
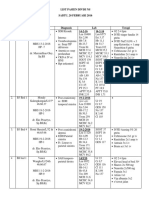
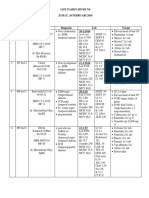
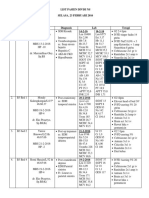
- List Pasien Divisi Bedah Plastik Kamis 17 MARET 2016 Jumlah Pasien: 7 PasienDocument2 pagesList Pasien Divisi Bedah Plastik Kamis 17 MARET 2016 Jumlah Pasien: 7 PasienasddfggPas encore d'évaluation
- List NS 20-2Document2 pagesList NS 20-2asddfggPas encore d'évaluation
- List Pasien Divisi Thovask 11 FebDocument3 pagesList Pasien Divisi Thovask 11 FebasddfggPas encore d'évaluation
- List Onko 29januariDocument6 pagesList Onko 29januariasddfggPas encore d'évaluation
- List Pasien Divisi Ns Jumat, 26 Februari 2016 Irina A Bawah: 4 Pasien No Kamar Identitas Diagnosis Lab Terapi 20-2-2016Document2 pagesList Pasien Divisi Ns Jumat, 26 Februari 2016 Irina A Bawah: 4 Pasien No Kamar Identitas Diagnosis Lab Terapi 20-2-2016asddfggPas encore d'évaluation
- List NS 23-2Document3 pagesList NS 23-2asddfggPas encore d'évaluation
- J NeurosurgDocument11 pagesJ NeurosurgasddfggPas encore d'évaluation
- Referensi 50Document3 pagesReferensi 50asddfggPas encore d'évaluation
- List NS 20-2Document2 pagesList NS 20-2asddfggPas encore d'évaluation
- CAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentDocument35 pagesCAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentAnonymous KgUtPlkjPas encore d'évaluation
- Drug AddictionDocument2 pagesDrug Addictionbokaneg100% (1)
- European Journal of Education Studies: Misango Nathan Chapia, Mwaura Kimani, Naftali RopDocument13 pagesEuropean Journal of Education Studies: Misango Nathan Chapia, Mwaura Kimani, Naftali RopgurubydesignPas encore d'évaluation
- FULL Download Ebook PDF Health Psychology An Interdisciplinary Approach 3rd Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Health Psychology An Interdisciplinary Approach 3rd Edition PDF Ebookkevin.saenz617100% (33)
- Treating Yourself Magazine #21Document132 pagesTreating Yourself Magazine #21murciano207Pas encore d'évaluation
- Jurnal BenzodiazepinDocument8 pagesJurnal Benzodiazepinkoasanak soreangPas encore d'évaluation
- Mental Health Implications of Discrimination Against Indigenous People - Ongoing Impact of The Canadian Indian Residential School SystemDocument20 pagesMental Health Implications of Discrimination Against Indigenous People - Ongoing Impact of The Canadian Indian Residential School SystemAashish GuptaPas encore d'évaluation
- Annual Report: Ngunu ZiroDocument11 pagesAnnual Report: Ngunu ZiroTage KannoPas encore d'évaluation
- Campaign Against DrugsDocument2 pagesCampaign Against DrugsJamina P. JamalodingPas encore d'évaluation
- Measuring Television AddictionDocument24 pagesMeasuring Television Addictionciprian72100% (1)
- Albrecht EQWLS Survey QNRDocument8 pagesAlbrecht EQWLS Survey QNRginutza88Pas encore d'évaluation
- Why Mental Health Professionals Avoid Self CareDocument3 pagesWhy Mental Health Professionals Avoid Self CareNereaPas encore d'évaluation
- Applicant's Name Interviewer's Name Date Answer Interviewer Notes Please Check The Box That ApplyDocument4 pagesApplicant's Name Interviewer's Name Date Answer Interviewer Notes Please Check The Box That ApplyAhmad Suhaemi93Pas encore d'évaluation
- Feedback XI G PRA MID-TERM EP 2Document8 pagesFeedback XI G PRA MID-TERM EP 2Syifa KamilaPas encore d'évaluation
- Factors Contributing To High Alcoholism Among Youths in Adumi Village, Arua District UgandaDocument17 pagesFactors Contributing To High Alcoholism Among Youths in Adumi Village, Arua District UgandaKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Level 1 Measure Child Age 11 To 17Document3 pagesLevel 1 Measure Child Age 11 To 17waleskacrzPas encore d'évaluation
- Mid Term VictimologyDocument3 pagesMid Term VictimologySubhojit Das0% (1)
- NSTP 1 Drugs EducationDocument32 pagesNSTP 1 Drugs EducationGianne Ina Castillo0% (3)
- Wet House - Stephanie McIntyre - Churchill Report 2009Document21 pagesWet House - Stephanie McIntyre - Churchill Report 2009New Zealand Social Entrepreneur Fellowship - PDF LibraryPas encore d'évaluation
- HLTH 1050 ReflectionDocument2 pagesHLTH 1050 Reflectionapi-242274352Pas encore d'évaluation
- Depression at WorkDocument14 pagesDepression at WorkMiguel Angulo JaraPas encore d'évaluation
- Drug Treatment Services For Adult Offenders - The State of The StateDocument16 pagesDrug Treatment Services For Adult Offenders - The State of The StateJeon MiaPas encore d'évaluation
- Question Bank-Clinical Toxicology Iv Pharm.D CHAPTER 1: General Principles Involved in The Management of Poisoning 3 Hrs II Short Essays: 5 MarksDocument10 pagesQuestion Bank-Clinical Toxicology Iv Pharm.D CHAPTER 1: General Principles Involved in The Management of Poisoning 3 Hrs II Short Essays: 5 MarksAnoop TandurPas encore d'évaluation
- Meth Minutes 2009Document9 pagesMeth Minutes 2009Peer Coach Academy Colorado100% (1)
- Clinical Case Report No 2Document11 pagesClinical Case Report No 2ملک محمد صابرشہزاد50% (2)
- Activity Sheets in HEALTH 2nd QUARTERDocument5 pagesActivity Sheets in HEALTH 2nd QUARTERArlene Beltran - SevillenaPas encore d'évaluation
- A Short Course in PsychiatryDocument151 pagesA Short Course in PsychiatryTijana Stevic100% (1)
- Coping With The Stress of COVID19Document4 pagesCoping With The Stress of COVID19LansingStateJournal100% (1)