Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Department of Labor: Errd SWDocument151 pagesDepartment of Labor: Errd SWUSA_DepartmentOfLaborPas encore d'évaluation
- Project Management ConsultantDocument11 pagesProject Management ConsultantsantoshmgurjarPas encore d'évaluation
- References - International Student StudiesDocument5 pagesReferences - International Student StudiesSTAR ScholarsPas encore d'évaluation
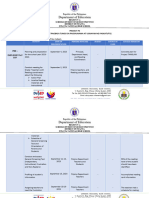
- Action Plan ReadingDocument7 pagesAction Plan ReadingRaymark sanchaPas encore d'évaluation
- RIZAL Summary Chapter 1-5Document10 pagesRIZAL Summary Chapter 1-5Jemnerey Cortez-Balisado CoPas encore d'évaluation
- 7 Effective Teaching Strategies For The ClassroomDocument4 pages7 Effective Teaching Strategies For The Classroomlea bendijo33% (3)
- Bauhaus Building, GropiusDocument3 pagesBauhaus Building, Gropiusivicanikolic100% (2)
- Stem Whitepaper Developing Academic VocabDocument8 pagesStem Whitepaper Developing Academic VocabKainat BatoolPas encore d'évaluation
- Unpacking Learning CompetenciesDocument16 pagesUnpacking Learning CompetenciesAngela BonaobraPas encore d'évaluation
- Introduction To Research Track 230221Document24 pagesIntroduction To Research Track 230221Bilramzy FakhrianPas encore d'évaluation
- Organisational Behaviour PDFDocument129 pagesOrganisational Behaviour PDFHemant GuptaPas encore d'évaluation
- IB Grade Boundaries May 2016Document63 pagesIB Grade Boundaries May 2016kostasPas encore d'évaluation
- Scholarship Application Form: TBS - Scholarships@tcd - IeDocument2 pagesScholarship Application Form: TBS - Scholarships@tcd - IeRoney GeorgePas encore d'évaluation
- Daniel B. Pe A Memorial College Foundation, Inc. Tabaco CityDocument3 pagesDaniel B. Pe A Memorial College Foundation, Inc. Tabaco CityAngelica CaldeoPas encore d'évaluation
- The University: AccreditationDocument9 pagesThe University: Accreditationbob cellPas encore d'évaluation
- Modular/Block Teaching: Practices and Challenges at Higher Education Institutions of EthiopiaDocument16 pagesModular/Block Teaching: Practices and Challenges at Higher Education Institutions of EthiopiaMichelle RubioPas encore d'évaluation
- Case StudyDocument3 pagesCase Studyapi-242748507100% (1)
- AAA Oral Communication Syllabus OkDocument3 pagesAAA Oral Communication Syllabus OkngocbummyPas encore d'évaluation
- Shine Candidates 1669027750Document20 pagesShine Candidates 1669027750Rohan DilawarPas encore d'évaluation
- Critique Paper No.2 Rizal in The Context of 19th Century PhilippinesDocument3 pagesCritique Paper No.2 Rizal in The Context of 19th Century PhilippinesMalia PolintanPas encore d'évaluation
- SUPO UbD The Giver Gr8 Szukielowicz 2014Document10 pagesSUPO UbD The Giver Gr8 Szukielowicz 2014MERVE TÜRKPas encore d'évaluation
- English Vi October 29Document3 pagesEnglish Vi October 29Catherine RenantePas encore d'évaluation
- Parenting Style Assessment PDFDocument4 pagesParenting Style Assessment PDFAbyssman ManPas encore d'évaluation
- Virginia Spanish 2 SyllabusDocument2 pagesVirginia Spanish 2 Syllabuskcoles1987Pas encore d'évaluation
- Unit II An Annotated OutlineDocument2 pagesUnit II An Annotated Outlineapi-420082848Pas encore d'évaluation
- Curriculum Map - Math8Document5 pagesCurriculum Map - Math8api-242927075Pas encore d'évaluation
- Power ElectronicsDocument107 pagesPower ElectronicsMr. VenkateshPas encore d'évaluation
- 9th Math (Arts Group) Unit 5 Solved NotesDocument26 pages9th Math (Arts Group) Unit 5 Solved NotesAsad Ali MeharPas encore d'évaluation
- Effective Difficult Conversations A Step-By-Step GuideDocument129 pagesEffective Difficult Conversations A Step-By-Step GuidechocobrowniePas encore d'évaluation
- Story15 HouseDocument29 pagesStory15 HousePAKK(SK,SJKT)-0619 Irene Wong Yen LingPas encore d'évaluation