Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Dka GuidelineDocument16 pagesDka GuidelineGhada HusseinPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Laporan Pagi Anestesi Operasi ElektifDocument2 pagesLaporan Pagi Anestesi Operasi ElektifAnnandra RahmanPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Pokemonnn AdvancedDocument1 pagePokemonnn AdvancedAnnandra RahmanPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Dka GuidelineDocument16 pagesDka GuidelineGhada HusseinPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Laporan Pagi Anestesi Operasi ElektifDocument2 pagesLaporan Pagi Anestesi Operasi ElektifAnnandra RahmanPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Laporan Pagi Anestesi Operasi ElektifDocument2 pagesLaporan Pagi Anestesi Operasi ElektifAnnandra RahmanPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Data DR Renny Buat BeliauDocument3 pagesData DR Renny Buat BeliauAnnandra RahmanPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Laporan Pagi Anestesi Operasi ElektifDocument2 pagesLaporan Pagi Anestesi Operasi ElektifAnnandra RahmanPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Common Otolaryngology Emergency Room Consults Michael Chao July 8, 2004Document15 pagesCommon Otolaryngology Emergency Room Consults Michael Chao July 8, 2004Annandra RahmanPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- WWW - Radarbanjarmasin.co .Id Iklan@radarbanjarmasin - Co .Id: Kantor Biro BanjarmasinDocument7 pagesWWW - Radarbanjarmasin.co .Id Iklan@radarbanjarmasin - Co .Id: Kantor Biro BanjarmasinVpn LegacyPas encore d'évaluation
- ATLS1Document36 pagesATLS1Ricardo Kuptios100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Laporan Pagi Anestesi Operasi ElektifDocument2 pagesLaporan Pagi Anestesi Operasi ElektifAnnandra RahmanPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Chest XDocument8 pagesChest XAnnandra RahmanPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Artropoda Beracun: Dr. ISTIANA, M.Kes Bagian/Lab. Parasitologi FK UnlamDocument56 pagesArtropoda Beracun: Dr. ISTIANA, M.Kes Bagian/Lab. Parasitologi FK UnlamRahmad Budi PrasetyoPas encore d'évaluation
- 23 FullDocument7 pages23 FullAnnandra RahmanPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- DapusDocument2 pagesDapusAnnandra RahmanPas encore d'évaluation
- Bifid Median Nerve in Patients With Carpal Tunnel SyndromeDocument8 pagesBifid Median Nerve in Patients With Carpal Tunnel SyndromeAnnandra RahmanPas encore d'évaluation
- 37 FullDocument6 pages37 FullAnnandra RahmanPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- BMC Public Health: Risk Factors For Operated Carpal Tunnel Syndrome: A Multicenter Population-Based Case-Control StudyDocument15 pagesBMC Public Health: Risk Factors For Operated Carpal Tunnel Syndrome: A Multicenter Population-Based Case-Control StudyAnnandra RahmanPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Pathology of The Ulnar Nerve in Acromegaly: PatientsDocument5 pagesThe Pathology of The Ulnar Nerve in Acromegaly: PatientsAnnandra RahmanPas encore d'évaluation
- Cheat 2k12Document3 pagesCheat 2k12Annandra RahmanPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Command Zero HourDocument19 pagesCommand Zero HourAnnandra RahmanPas encore d'évaluation
- cnc4 Walkhtrough2Document27 pagescnc4 Walkhtrough2Annandra RahmanPas encore d'évaluation
- Eur J Heart Fail 2009 Hawkins 292 8Document7 pagesEur J Heart Fail 2009 Hawkins 292 8Annandra RahmanPas encore d'évaluation
- Cari Di You TubetxtDocument1 pageCari Di You TubetxtAnnandra RahmanPas encore d'évaluation
- Multiple Myeloma in IndonesiaDocument6 pagesMultiple Myeloma in IndonesiaAnctho LukmiPas encore d'évaluation
- Cadmium Accumulation in The Main Organs During A Chronic ExposureDocument12 pagesCadmium Accumulation in The Main Organs During A Chronic ExposureAnnandra RahmanPas encore d'évaluation
- 1436Document10 pages1436Annandra RahmanPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Inversio UteriDocument4 pagesInversio UteriJokevin PrasetyadhiPas encore d'évaluation
- Negative IonDocument2 pagesNegative IonDekzie Flores MimayPas encore d'évaluation
- Married Women of Reproductive AgeDocument26 pagesMarried Women of Reproductive Agelibagon rhuPas encore d'évaluation
- Shantaes SurprisingDocument7 pagesShantaes SurprisingMitchPas encore d'évaluation
- Spontaneous Abortion PPDocument47 pagesSpontaneous Abortion PPSurgeon Raza HamidPas encore d'évaluation
- Obstetric Sample Questions With RationaleDocument31 pagesObstetric Sample Questions With RationaleTomzki Cornelio50% (2)
- Antepartum HemorrhageDocument31 pagesAntepartum HemorrhageChristianahPas encore d'évaluation
- Thai PF 31.3.23Document11 pagesThai PF 31.3.23gaurav sharmaPas encore d'évaluation
- Breast Shape Yoga PosesDocument4 pagesBreast Shape Yoga Posessubscribe_allPas encore d'évaluation
- Case Summary Ovarian CystDocument4 pagesCase Summary Ovarian CystFrancesca AkanjiPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Myoma, EndometriosisDocument57 pagesMyoma, EndometriosisSashka Evtodieva100% (1)
- Cervical Insufficiency + Cord PresentationDocument2 pagesCervical Insufficiency + Cord PresentationMSPas encore d'évaluation
- Last Module in The Midterm PeriodDocument11 pagesLast Module in The Midterm PeriodCheskah sinangotePas encore d'évaluation
- Tugas Mandiri Pertemuan 8 Askeb Pada Kasus Kompleks (2) - CompressedDocument31 pagesTugas Mandiri Pertemuan 8 Askeb Pada Kasus Kompleks (2) - CompressedArkan SariPas encore d'évaluation
- ფიზიოლოგიური მშობიარობის მართვაDocument30 pagesფიზიოლოგიური მშობიარობის მართვაAchi BeridzePas encore d'évaluation
- Kanda - Histology of The Male Reproductive Organs-1Document3 pagesKanda - Histology of The Male Reproductive Organs-1y yasminPas encore d'évaluation
- CPG Malaysia - Management of MenorrhagiaDocument22 pagesCPG Malaysia - Management of MenorrhagiaziggyshahdustPas encore d'évaluation
- 2023 Buntis Congress Training DesignDocument3 pages2023 Buntis Congress Training DesignBeverly Calma100% (4)
- Cmca Lec MidtermDocument43 pagesCmca Lec MidtermKate Onniel RimandoPas encore d'évaluation
- FETOMATERNAL WARD REPORT 6 Feb 2 PatDocument59 pagesFETOMATERNAL WARD REPORT 6 Feb 2 PatMegaSariDewiPas encore d'évaluation
- Combined List of TitlesDocument13 pagesCombined List of Titlesmad kingPas encore d'évaluation
- Gestational DiabetesDocument6 pagesGestational DiabetesZAY EMPas encore d'évaluation
- Addendum ALSO Tanzania RevisedDocument43 pagesAddendum ALSO Tanzania RevisedviaereaPas encore d'évaluation
- Advances in Reproductive EndocrinologyDocument41 pagesAdvances in Reproductive Endocrinologyapi-3705046Pas encore d'évaluation
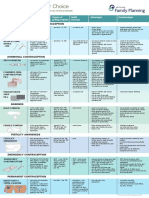
- Contraception Options in New ZealandDocument2 pagesContraception Options in New ZealandStuff NewsroomPas encore d'évaluation
- Kumpulan Jurnal Dan SumberDocument22 pagesKumpulan Jurnal Dan Sumberlina herlinaPas encore d'évaluation
- (Gender and Well-Being.) Ortiz, Teresa - Santesmases, María Jesús - Gendered Drugs and Medicine - Historical and Socio-Cultural Perspectives-Ashgate Publishing Limited (2014)Document261 pages(Gender and Well-Being.) Ortiz, Teresa - Santesmases, María Jesús - Gendered Drugs and Medicine - Historical and Socio-Cultural Perspectives-Ashgate Publishing Limited (2014)Federico AnticapitalistaPas encore d'évaluation
- Contraceptiv WilliamDocument85 pagesContraceptiv WilliamPridina SyadirahPas encore d'évaluation
- ObGyn Outline BeckmannDocument85 pagesObGyn Outline Beckmannp4sierra50% (2)
- Step 2 CK Usmle Questions For Ob GynDocument48 pagesStep 2 CK Usmle Questions For Ob Gyniamdonut87% (15)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesD'EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesÉvaluation : 5 sur 5 étoiles5/5 (70)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeD'EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeÉvaluation : 3.5 sur 5 étoiles3.5/5 (13)
- An Autobiography of Trauma: A Healing JourneyD'EverandAn Autobiography of Trauma: A Healing JourneyÉvaluation : 5 sur 5 étoiles5/5 (2)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryD'EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryÉvaluation : 4.5 sur 5 étoiles4.5/5 (157)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisD'EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisÉvaluation : 3 sur 5 étoiles3/5 (2)