Vous aimerez peut-être aussi
- CRP Is A Mediator of CV DiseaseDocument9 pagesCRP Is A Mediator of CV DiseaseleozdmPas encore d'évaluation
- Ni Hmsdasads 34581Document11 pagesNi Hmsdasads 34581Joe AjaPas encore d'évaluation
- Causes of Changes in Carotid Intima-Media Thickness: A Literature ReviewDocument10 pagesCauses of Changes in Carotid Intima-Media Thickness: A Literature ReviewSorin ParalescuPas encore d'évaluation
- Effect of Cystatin C To Sistolic Dan Diastolic Blood Pressure in Elderly With Normal Renal FunctionDocument5 pagesEffect of Cystatin C To Sistolic Dan Diastolic Blood Pressure in Elderly With Normal Renal FunctionERLINA MARFIANTI dr.Pas encore d'évaluation
- C Protein and MortalityDocument9 pagesC Protein and MortalityopaolisPas encore d'évaluation
- 302 Cardiovascular Risk: AssessmentDocument1 page302 Cardiovascular Risk: AssessmentLêHữuHoàiPas encore d'évaluation
- PDF 9Document8 pagesPDF 9OulnstPas encore d'évaluation
- Chronic Kidney Disease and Its ComplicationsDocument6 pagesChronic Kidney Disease and Its ComplicationsmedicalPas encore d'évaluation
- Human C-Reactive Protein and The Metabolic SyndromeDocument13 pagesHuman C-Reactive Protein and The Metabolic SyndromeEmir SaricPas encore d'évaluation
- Serum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenDocument15 pagesSerum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenEcha MagungPas encore d'évaluation
- Nejm Pcsk9 StudyDocument10 pagesNejm Pcsk9 Studyherbertgur777Pas encore d'évaluation
- Ference BA Et Al. N Eng J Med 2016Document56 pagesFerence BA Et Al. N Eng J Med 2016Juan Manuel UrbanoPas encore d'évaluation
- 116 229 1 SMDocument6 pages116 229 1 SMsinlookerPas encore d'évaluation
- C-Reactive Protein and Cardiovascular Diseases-Is It Ready For Primetime?Document7 pagesC-Reactive Protein and Cardiovascular Diseases-Is It Ready For Primetime?dastgirrajaPas encore d'évaluation
- Changes in Plasma Fibrinogen, Homocysteine and Lipid Profile in Coronary Artery Disease Patients of North Indian (Punjab) Popu-LationDocument4 pagesChanges in Plasma Fibrinogen, Homocysteine and Lipid Profile in Coronary Artery Disease Patients of North Indian (Punjab) Popu-LationMaya RustamPas encore d'évaluation
- Rosuvastatia y PCR en ScaDocument3 pagesRosuvastatia y PCR en ScaWilliankmachoPas encore d'évaluation
- Clinical Use of Carotid Intima-Media Thickness: Review of The LiteratureDocument8 pagesClinical Use of Carotid Intima-Media Thickness: Review of The LiteraturehardianPas encore d'évaluation
- C-Reactive Protein and The Prediction of Cardiovascular Events Among Those at Intermediate RiskDocument17 pagesC-Reactive Protein and The Prediction of Cardiovascular Events Among Those at Intermediate RiskMarisol GonzalezPas encore d'évaluation
- Jupiter Crestor StudyDocument13 pagesJupiter Crestor StudyJim BuckPas encore d'évaluation
- Use of Statins and The Incidence of Type 2 Diabetes MellitusDocument6 pagesUse of Statins and The Incidence of Type 2 Diabetes MellitusBenji MincholaPas encore d'évaluation
- C Reaktive ProteinDocument4 pagesC Reaktive Proteinsinggih2008Pas encore d'évaluation
- Learning Insight LauderdaleDocument3 pagesLearning Insight LauderdaleDale DeocaresPas encore d'évaluation
- Cohorta NEJMfjaslnfjdlalkeDocument9 pagesCohorta NEJMfjaslnfjdlalkeAndrei VasilescuPas encore d'évaluation
- Lipid Biomarker To Predict Coronary DiseasesDocument10 pagesLipid Biomarker To Predict Coronary DiseasesNeha MasarkarPas encore d'évaluation
- Framingham PaperDocument6 pagesFramingham PaperLikhna PertiwiPas encore d'évaluation
- Oup Accepted Manuscript 2020Document11 pagesOup Accepted Manuscript 2020Luis Bonino SanchezPas encore d'évaluation
- Cardiovascular Risk Factors in Patients With Chronic Kidney Disease Under Conservative TreatmentDocument9 pagesCardiovascular Risk Factors in Patients With Chronic Kidney Disease Under Conservative TreatmentTai rascunhos TaiPas encore d'évaluation
- Hormone Therapy and Cardiovascular DiseaseDocument7 pagesHormone Therapy and Cardiovascular Diseaseosama saeedPas encore d'évaluation
- Nam 2011Document6 pagesNam 2011Ahmed AnwarPas encore d'évaluation
- Effects of Candesartan and Amlodipine On Cardiovascular Events in Hypertensive Patients With Chronic Kidney DiseaseDocument8 pagesEffects of Candesartan and Amlodipine On Cardiovascular Events in Hypertensive Patients With Chronic Kidney Diseasenova sorayaPas encore d'évaluation
- Glycosylated ProteinsDocument5 pagesGlycosylated ProteinsRonyPas encore d'évaluation
- CKD Ska2Document14 pagesCKD Ska2Maya RustamPas encore d'évaluation
- Andesty CantikDocument13 pagesAndesty Cantiklim andestyPas encore d'évaluation
- Correlates of Acute Insulin Resistance in The Early Phase of Non-Diabetic ST-elevation Myocardial InfarctionDocument9 pagesCorrelates of Acute Insulin Resistance in The Early Phase of Non-Diabetic ST-elevation Myocardial InfarctionmeliabudiPas encore d'évaluation
- Children AherosclerosisDocument7 pagesChildren AherosclerosisIuliana SovaPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptRohmantuah_Tra_1826Pas encore d'évaluation
- AURORA: Is There A Role For Statin Therapy in Dialysis Patients?Document4 pagesAURORA: Is There A Role For Statin Therapy in Dialysis Patients?Ravan WidiPas encore d'évaluation
- Índice de Castelli - Summary Estimates of Cholesterol UsedDocument6 pagesÍndice de Castelli - Summary Estimates of Cholesterol UsedmartaacPas encore d'évaluation
- Plasma Concentration of C-Reactive Protein and Risk of Developing Peripheral Vascular DiseaseDocument8 pagesPlasma Concentration of C-Reactive Protein and Risk of Developing Peripheral Vascular Diseaseashphoenix32Pas encore d'évaluation
- Pi Is 0140673610604849Document8 pagesPi Is 0140673610604849Montserrat Duran TorreblancaPas encore d'évaluation
- Artikel 2Document9 pagesArtikel 2Uli DoankPas encore d'évaluation
- Rodrigues 2010Document7 pagesRodrigues 2010Илија РадосављевићPas encore d'évaluation
- High Density Lipoprotein Cholesterol, Total Cholesterol Screening, and Myocardial InfarctionDocument5 pagesHigh Density Lipoprotein Cholesterol, Total Cholesterol Screening, and Myocardial InfarctionChristian Ivan SantosoPas encore d'évaluation
- Higado Graso No Alcoholico y Niveles de PCRDocument6 pagesHigado Graso No Alcoholico y Niveles de PCRperuliz19Pas encore d'évaluation
- 3.cardiovascular Risk Stratification and Appropriate Use of Statins in Patients With Systemic Lupus Erythematosus According To Different StrategiesDocument8 pages3.cardiovascular Risk Stratification and Appropriate Use of Statins in Patients With Systemic Lupus Erythematosus According To Different StrategiesSilvia PeresPas encore d'évaluation
- Kunutsor - 2016 - Serum Zinc Concentrations and Incident HypertensionDocument7 pagesKunutsor - 2016 - Serum Zinc Concentrations and Incident Hypertensionzi coPas encore d'évaluation
- Keywords:-Acute Coronary Syndrome, Triglycerides, HighDocument6 pagesKeywords:-Acute Coronary Syndrome, Triglycerides, HighInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- NAFLD and Non-Liver ComorbiditiesDocument21 pagesNAFLD and Non-Liver ComorbiditiesGestne AurePas encore d'évaluation
- Review Article: Investigation On Cardiovascular Risk Prediction Using Physiological ParametersDocument22 pagesReview Article: Investigation On Cardiovascular Risk Prediction Using Physiological ParametersNnaemeka NwobodoPas encore d'évaluation
- Association Between Acute Myocardial Infarction, Lipid Profile and Smoking HabitDocument5 pagesAssociation Between Acute Myocardial Infarction, Lipid Profile and Smoking HabitIOSRjournalPas encore d'évaluation
- ,content, 31,2,361 FullDocument2 pages,content, 31,2,361 FullMilka MimingPas encore d'évaluation
- Research Open Access: Dai Et Al. Lipids in Health and Disease (2019) 18:210Document8 pagesResearch Open Access: Dai Et Al. Lipids in Health and Disease (2019) 18:210drewantaPas encore d'évaluation
- Accepted Manuscript: 10.1016/j.jacl.2017.02.017Document34 pagesAccepted Manuscript: 10.1016/j.jacl.2017.02.017ochaPas encore d'évaluation
- Comparison of C-Reactive Protein and Low-Density LipoproteinDocument9 pagesComparison of C-Reactive Protein and Low-Density LipoproteinJason GossPas encore d'évaluation
- 1774 Full PDFDocument7 pages1774 Full PDFhfathiardiPas encore d'évaluation
- 25rakshitha EtalDocument8 pages25rakshitha EtaleditorijmrhsPas encore d'évaluation
- 2019 Article 612Document17 pages2019 Article 612Asad NawazPas encore d'évaluation
- Cardiovascular Risk in Obese Patients With Chronic PeriodontitisDocument8 pagesCardiovascular Risk in Obese Patients With Chronic PeriodontitisThais DezemPas encore d'évaluation
- Euu 2Document10 pagesEuu 2Johanna GalvisPas encore d'évaluation
- 1R26999 Fluitest® GGT R1-GB-en 2014-05-16Document5 pages1R26999 Fluitest® GGT R1-GB-en 2014-05-16Maya RustamPas encore d'évaluation
- 02 WholeDocument173 pages02 WholeMaya RustamPas encore d'évaluation
- 1R26999 Fluitest® GGT R1-GB-en 2014-05-16Document5 pages1R26999 Fluitest® GGT R1-GB-en 2014-05-16Maya RustamPas encore d'évaluation
- Baron CH Introduction To VirologyDocument2 pagesBaron CH Introduction To VirologyneysaonlinePas encore d'évaluation
- 6Document8 pages6Maya RustamPas encore d'évaluation
- 01-2009 EASD C-Peptide Poster 580Document1 page01-2009 EASD C-Peptide Poster 580Maya RustamPas encore d'évaluation
- Amylase UrinDocument3 pagesAmylase UrinMaya RustamPas encore d'évaluation
- Agrmicral 9Document13 pagesAgrmicral 9Maya RustamPas encore d'évaluation
- 01-2009 EASD C-Peptide Poster 580Document1 page01-2009 EASD C-Peptide Poster 580Maya RustamPas encore d'évaluation
- Rates of Positive Cardiac Troponin I and Creatine Kinase MB Mass Among Patients Hospitalized For Suspected Acute Coronary SyndromesDocument6 pagesRates of Positive Cardiac Troponin I and Creatine Kinase MB Mass Among Patients Hospitalized For Suspected Acute Coronary SyndromesMaya RustamPas encore d'évaluation
- D M P S: Ecision Aking and Roblem OlvingDocument6 pagesD M P S: Ecision Aking and Roblem OlvingMaya RustamPas encore d'évaluation
- Doi:10.1016/j.jacc.2009.01.016 2009 53 A198-A230: Hypertension, Lipids and PreventionDocument35 pagesDoi:10.1016/j.jacc.2009.01.016 2009 53 A198-A230: Hypertension, Lipids and PreventionMaya RustamPas encore d'évaluation
- Neumaier 1998 Fundamentals Quality Assessment Molecular Ampli MethodDocument15 pagesNeumaier 1998 Fundamentals Quality Assessment Molecular Ampli MethodMaya RustamPas encore d'évaluation
- 11 MutagenesisDocument8 pages11 MutagenesisMaya RustamPas encore d'évaluation
- Jurnal Malaria TesDocument5 pagesJurnal Malaria TesMaya RustamPas encore d'évaluation
- Jurnal New Cut Falue TransferinDocument4 pagesJurnal New Cut Falue TransferinMaya RustamPas encore d'évaluation
- Amino Acid 2009Document7 pagesAmino Acid 2009Maya RustamPas encore d'évaluation
- Parsons 2002 TBC PCRDocument7 pagesParsons 2002 TBC PCRMaya RustamPas encore d'évaluation
- Eur Heart J 2000 Thambyrajah 967 74Document8 pagesEur Heart J 2000 Thambyrajah 967 74Angga Maulana IbrahimPas encore d'évaluation
- Jurnal AlbuminDocument6 pagesJurnal AlbuminMaya RustamPas encore d'évaluation
- Adiponektin 1Document8 pagesAdiponektin 1Maya RustamPas encore d'évaluation
- AbstractDocument1 pageAbstractMaya RustamPas encore d'évaluation
- Jurnal AdipokineDocument9 pagesJurnal AdipokineMaya RustamPas encore d'évaluation
- Homosistein AMIDocument7 pagesHomosistein AMIMaya RustamPas encore d'évaluation
- Tesis AdiponektinDocument6 pagesTesis AdiponektinMaya RustamPas encore d'évaluation
- Changes in Plasma Fibrinogen, Homocysteine and Lipid Profile in Coronary Artery Disease Patients of North Indian (Punjab) Popu-LationDocument4 pagesChanges in Plasma Fibrinogen, Homocysteine and Lipid Profile in Coronary Artery Disease Patients of North Indian (Punjab) Popu-LationMaya RustamPas encore d'évaluation
- Homosistein AMIDocument7 pagesHomosistein AMIMaya RustamPas encore d'évaluation
- Homocysteine and Markers of Coagulation and Endothelial Cell ActivationDocument7 pagesHomocysteine and Markers of Coagulation and Endothelial Cell ActivationMaya RustamPas encore d'évaluation
- Homo Cyst EineDocument15 pagesHomo Cyst EineMaya RustamPas encore d'évaluation
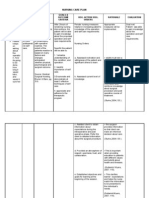
- NCP 1Document4 pagesNCP 1Ke EjiePas encore d'évaluation
- War Dogs 1Document26 pagesWar Dogs 1api-340421195Pas encore d'évaluation
- Dry Needling in Lateral Epicondylitis A Prospective EBP PDFDocument5 pagesDry Needling in Lateral Epicondylitis A Prospective EBP PDFDanielle Denice LacabaPas encore d'évaluation
- 4.1 - Common Nutritional Problems in ToddlersDocument6 pages4.1 - Common Nutritional Problems in ToddlersDrSajid BuzdarPas encore d'évaluation
- Philhealth Cf4 2017-2018Document8 pagesPhilhealth Cf4 2017-2018Julius Yves Dulfo BagacayPas encore d'évaluation
- Sialography ExaminationDocument14 pagesSialography ExaminationEkaRahmaPas encore d'évaluation
- Jaclyn Wanie Resume PDFDocument2 pagesJaclyn Wanie Resume PDFapi-631931479Pas encore d'évaluation
- Iron Deficiency AnemiaDocument25 pagesIron Deficiency AnemiaDetria Rahma GastiPas encore d'évaluation
- COCONUT OIL 101 Miraculous Coconut Oil Benefits Cures Uses and Remedies by Victoria Lane PDFDocument22 pagesCOCONUT OIL 101 Miraculous Coconut Oil Benefits Cures Uses and Remedies by Victoria Lane PDFedwinw18Pas encore d'évaluation
- An Exploratory BriefDocument11 pagesAn Exploratory BriefElizabeth Roxan Lizaso GonzálezPas encore d'évaluation
- Siddha Medicines For Bronchial AsthmaDocument9 pagesSiddha Medicines For Bronchial AsthmasalemraghuPas encore d'évaluation
- Definitive Orthodontic Treatmen1Document2 pagesDefinitive Orthodontic Treatmen1Dr.Fadi86% (7)
- 3rd Care of The Critically Ill Surgical Patient PDFDocument273 pages3rd Care of The Critically Ill Surgical Patient PDFPavitra RamasamyPas encore d'évaluation
- Case Study - La Roche-Posay Media Gathering 2006Document3 pagesCase Study - La Roche-Posay Media Gathering 2006Lhcmkt LhcPas encore d'évaluation
- Healthy Food PDFDocument8 pagesHealthy Food PDFnurul syafizatul shahirahPas encore d'évaluation
- Otitis MediaDocument11 pagesOtitis MediajessyPas encore d'évaluation
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Document4 pagesComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangPas encore d'évaluation
- Document Dynasand Phosphorus Removal Case Study 1788Document1 pageDocument Dynasand Phosphorus Removal Case Study 1788taenker123Pas encore d'évaluation
- A Dictionary For Psychotherapists PDFDocument1 375 pagesA Dictionary For Psychotherapists PDFMonica100% (2)
- PMLS Lesson 4Document3 pagesPMLS Lesson 4Void MelromarcPas encore d'évaluation
- Kyasanur Forest DiseaseDocument2 pagesKyasanur Forest DiseaseGenoMacaraanPas encore d'évaluation
- Alcohol History Taking - Geeky MedicsDocument6 pagesAlcohol History Taking - Geeky MedicsJahangir AlamPas encore d'évaluation
- Glimpse of My ResearchDocument4 pagesGlimpse of My Researchमनोज जैनPas encore d'évaluation
- STSurg NumntDocument11 pagesSTSurg NumntrohiPas encore d'évaluation
- Acute Otitis Media (Ready) PPTDocument71 pagesAcute Otitis Media (Ready) PPTMegawati Abubakar100% (1)
- CDI Week Sept 2012Document2 pagesCDI Week Sept 2012RanoCenterPas encore d'évaluation
- Detoxification Therapeutics For Heavy Metals, Toxic Chemicals and Other NeurotoxinsDocument175 pagesDetoxification Therapeutics For Heavy Metals, Toxic Chemicals and Other Neurotoxins300r100% (9)
- A Re-Evaluation of Acting Out in Relation To Working ThroughDocument11 pagesA Re-Evaluation of Acting Out in Relation To Working ThroughUriel García VarelaPas encore d'évaluation
- Boils and Carbuncles: (Mayo Clinic)Document15 pagesBoils and Carbuncles: (Mayo Clinic)Jimmy ThomasPas encore d'évaluation
- Hypnosis - Gerald Kein - Little Known Secrets of A Successful Hypnotic SessionDocument4 pagesHypnosis - Gerald Kein - Little Known Secrets of A Successful Hypnotic SessionMaria Stroe86% (7)