Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Annabelle Tomlin Reflection PaperDocument7 pagesAnnabelle Tomlin Reflection Paperapi-557981712Pas encore d'évaluation
- Health Teaching PlanDocument11 pagesHealth Teaching PlanVic Intia Paa100% (1)
- Preventive MedicineDocument5 pagesPreventive Medicinescribdnotes123Pas encore d'évaluation
- History of Navy EntomologyDocument35 pagesHistory of Navy Entomologyrville1559Pas encore d'évaluation
- Rapid Diagnostic Testing For SARS-CoV-2Document9 pagesRapid Diagnostic Testing For SARS-CoV-2Wilfredo NuñezPas encore d'évaluation
- Experiencing The Lifespan 4th Edition by Belsky ISBN Test BankDocument40 pagesExperiencing The Lifespan 4th Edition by Belsky ISBN Test Bankshantel100% (23)
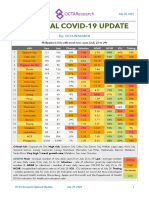
- National COVID-19 Update by Octa Research On July 30, 2021Document2 pagesNational COVID-19 Update by Octa Research On July 30, 2021RapplerPas encore d'évaluation
- Area C Cluster 10 Barangay Barualte AND Barangay Imelda: Tingao, Bandar - Ali I. Ventigan, Jonathan LDocument19 pagesArea C Cluster 10 Barangay Barualte AND Barangay Imelda: Tingao, Bandar - Ali I. Ventigan, Jonathan LjlventiganPas encore d'évaluation
- Social Medicine NotesDocument180 pagesSocial Medicine NotesAnonymous U2if0tPas encore d'évaluation
- Tangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationDocument3 pagesTangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationbenPas encore d'évaluation
- Guide To Successful Breastfeeding-BookletDocument16 pagesGuide To Successful Breastfeeding-Bookletandreeatalos100% (1)
- Historical Development of Community Health and Community HealthDocument107 pagesHistorical Development of Community Health and Community HealthHarini100% (1)
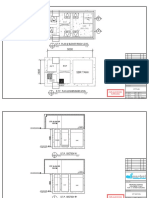
- Plan Plumbing DR Azam (Black)Document1 pagePlan Plumbing DR Azam (Black)Muhd HakimiePas encore d'évaluation
- Lack of Water Supply in Barangay Balagtas, Matag-Ob, LeyteDocument5 pagesLack of Water Supply in Barangay Balagtas, Matag-Ob, LeyteJedah V. BatisPas encore d'évaluation
- Community Acquired Pneumonia in Malaysia PDFDocument2 pagesCommunity Acquired Pneumonia in Malaysia PDFCassPas encore d'évaluation
- Eo 2021 004 Referral Psychosocial ServicesDocument2 pagesEo 2021 004 Referral Psychosocial ServicesWaldz Renales100% (1)
- COPARDocument109 pagesCOPARKrista CorpuzPas encore d'évaluation
- Safety of COVID-19 Vaccines - CDCDocument3 pagesSafety of COVID-19 Vaccines - CDCkelvinkinergyPas encore d'évaluation
- CPR DirectorynewDocument92 pagesCPR DirectorynewZyve AfricaPas encore d'évaluation
- Case Presewntation - C - SectionDocument12 pagesCase Presewntation - C - Sectionpriyanka50% (2)
- BHB Orientation For NDPs-1Document19 pagesBHB Orientation For NDPs-1Shevan Simon AliñabonPas encore d'évaluation
- Current Global Polio Situation and Polio Eradication ProgressDocument19 pagesCurrent Global Polio Situation and Polio Eradication ProgressDermawan SinagaPas encore d'évaluation
- Internal Policies And/Or Procedure (Ipp)Document2 pagesInternal Policies And/Or Procedure (Ipp)LENARD GRIJALDOPas encore d'évaluation
- STPDocument3 pagesSTPEdmar Bangayan0% (1)
- Set 1 - CommunityDocument31 pagesSet 1 - CommunityDefensor Pison GringgoPas encore d'évaluation
- Obs Gyn ClerkingDocument5 pagesObs Gyn ClerkingdonaldooiPas encore d'évaluation
- SQD FinalDocument30 pagesSQD FinalMohammed APas encore d'évaluation
- What Is A Clinical Trial?: BackgroundDocument8 pagesWhat Is A Clinical Trial?: BackgroundsenthilmnursePas encore d'évaluation
- GFP EnauDocument2 pagesGFP EnauDomenico BevilacquaPas encore d'évaluation
- Multiple GestationDocument22 pagesMultiple GestationIrish Ivy VibethPas encore d'évaluation