IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 11 Ver.X (Nov. 2015), PP 34-40
www.iosrjournals.org
Clinical Study of Benign Breast Diseases
1
Dr. B.V. Amruthavalli M.S., 2Dr. V. Srihari M.S.,
Asst.Prof of General Surgery Guntur Medical College, Guntur
Prof of General Surgery Kurnool Medical College, Kurnool
Abstract: This study of Benign Breast Diseases was done between 2008 2011 at Kurnool MedicalCollege and
Hospital, Kurnool. The study group consisted 175 patients between menarche to 50 yrs. This study chosen as
50-55% of women suffer from breast related disorder.Benign Breast Diseases which is most common cause of
breast problems with which Upto 30% of women suffer.
Background: The objectives was to study were to Study the BENIGN BREAST DISEASES with regard to
- Clinical presentation
- Age wise distribution
- Marital status and parity.
Methods: 175 female patients from Menarche upto 50 years who attended surgery out patient department
during 2008 to2011 at KURNOOL MEDICAL COLLEGE GOVERNMENT HOSPITAL, KURNOOL. With
various problems . 74 cases were diagnosed as BBD after triple assessment like
-clinical examination
-Ultra sonography or Mammography
-FNAC or Core Needle Biopsy
Were made within 72 HOURS from the first consultation.
Results: Out of 175 cases a total of 74 cases were found to be in study group . Fibroadenoma accounted for
43% which was highest in number.
Fibroadenosis was the next highest upto 31%
Breast Abscess about 18%
Mastitis 4%
Cystosarcoma Phyllodes and Duct Ectasia about 1.35%
Conclusion: BBD are common in females and FIBROADENOMA is the commonest in all. Triple assessment
provided a quick diagnosis and it alleviated unnecessary anxiety for the patients about breast cancer. The
clinical diagnosis of the breast lump as confirmed by cytology and histology was accurate in 91.95% of cases.
Key words:
-BBD, Risk factor
-Pathology, Triple assessment.
I.
Introduction
Benign Breast Diseases (BBDs) is a group of breast diseases which is not cancer. It is the most
common cause of breast problems in females and it is more frequent than the malignant ones [16]. In fact, it is
at least 10 times more common than breast cancer in the west [7]. Upto 30% of the women who suffer from
BBDs will require treatment at some time in their lives [8]. A triple assessment which is done by a clinical
examination, imaging like ultrasonography (USG) or mammography and a pathological examination FNAC or
core needle biopsy, during the initial consultation, allows a majority of the patients with discrete BBDs to be
given immediate reassurance. Since a majority of the benign lesions are not associated with an increased risk for
subsequent breast cancer, unnecessary surgical procedures can be avoided. Making an early diagnosis and
planning the treatment within 72 hours of the first consultation, helps in alleviating unnecessary anxiety about
breast cancer and those BBDs patients with an increased risk of malignancy like atypical hyperplasia, are given
a prompt treatment, a proper follow-up and awareness regarding the risk of breast cancer.
The popular classification of BBDs according to the Aberration of the Normal Development and
Involution (ANDI) causes confusion due to a lack of clarity in distinguishing between the normal physiological
changes and the pathologic ones. One of the more satisfying classifications would be the one which was devised
by Love S et al., [9], the so -called Nashville classification. According to this, BBDs is classified by 2 systems.
Pathologically, BBDs is divided into (a) non-proliferative lesions, (b) proliferative lesions Section without
atypical and(c) atypical proliferative lesions. Clinically, BBDs is classified as (a) physiologic swelling and
tenderness, (b) nodularity, (c) breast pain, (d) palpable lumps, (e) nipple discharge and (f) infections or
inflammation. In this study, we profiled the incidence of BBDs, the relative frequencies of the different types of
BBDs and their clinical features. Secondly, we attempted at correlating the clinical and pathological findings
DOI: 10.9790/0853-1411103440
www.iosrjournals.org
34 | Page
Clinical Study of Benign Breast Diseases
wherever possible.
II.
Materials And Methods
This descriptive study was conducted in the Out Patients Department of General Surgery in kurnool
Medical College, Kurnool,Andhra Pradesh from 2008 to 2011. The 74 women who were treated for BBDs
were included in this study. The patients were required to give written informed consents prior to their
enrolment in the study and a clearance was taken as per the institutes ethical committee guidelines.
Inclusion criteria
Female patients from menarche to 50 years with any benign disorder/disease of the breast-for example,
a breast lump, breast pain or a nipple discharge, were included.
Exclusion criteria
Women with an obvious malignant disease or those who had been treated for malignancy earlier, were
excluded in this study. .
A detailed history and a thorough physical examination were the basis of the study. After making an appropriate
clinical diagnosis, one or more of the special investigations FNAC, mammography, ultrasound or a coreneedle biopsy were carried out for the confirmation of the diagnosis.
The FNAC smears were reported by using standardized diagnostic criteria by the same pathologist and
they were categorized into non proliferative/proliferative without atypia/atypical proliferative lesion/frank
carcinoma. A routine histopathological examination was done for the core biopsy and the excision biopsy
samples and a cytological and histological-correlation was also done. The clinical diagnosis, particularly in the
case of the benign breast lumps, was compared with the cytological or the histological findings and the accuracy
of the clinical diagnosis was evaluated.
III.
Observation And Results
After detailed enquire into the history and thorough examination a provisional diagnosis was arrived at
and the patients were investigated into, excluding those women who were found normal. A total of 74 cases of
benign diseases were found in the study group.
The total number of benign diseases, the various provisional diagnoses arrived at clinically were as
follows:
Disease
Fibroadenoma
No.of cases
32
Percentage
43.24%
Fibroadenosis
23
31.08%
Mastitis
4.05%
Breast Abscess
14
18.91%
Cystocarcoma Phylloides
1.35%
Duct Ectasia
1.35%
74
Percentage of cases
1.35%
1.35%
Fibroadenoma
19%
43%
Fibroadenosis
Mastitis
4%
Breast Abscess
Cystocarcoma
Phylloides
31%
DOI: 10.9790/0853-1411103440
Duct Ectasia
www.iosrjournals.org
35 | Page
Clinical Study of Benign Breast Diseases
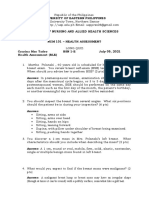
Age wise distribution of benign breast diseases in the 175 patients studied is as follows; 45 patients
were <20yrs. 69 patients were between 20-30yrs. 47 patients were between 30-40yrs. 18 patients were above
40yrs.
Age wise distribution of benign diseases in 175 cases
Age
Total no of females examined
<20
20-30
30-40
>40
42
69
46
18
165
No.of cases with benign breast
diseases
19
36
17
2
74
% of cases with benign breast
diseases
45.23%
52.17%
36.95%
11.11%
42.28%
No.of cases
Age wise distribution of benign
diseases
80
70
60
50
40
30
20
10
0
69
Total no of females
examined
46
42
36
No.of cases with benign
breast diseases
19
17
18
2
<20
20-30
30-40
>40
Age
Maximum numbers of patients with benign breast diseases in this study group were present in the age
groups of 20-30 yrs. (52.17%) followed by <20 yrs. (45.23%). More than 74% of the benign breast diseases
were in these two age groups.
Of the 42 patients in the age group of <20 yrs, 31 were unmarried and 11 were married. Of the 69
patients in the age group of 20-30 yrs. 17 were unmarried and 52 were married. Of the 46 patients in the age
group of 30-40yrs. one was unmarried and 45 were married and all the 18 patients in the age group >40yrs, were
married.
Marital status of the study group
Age
<20 yrs
20-30 yrs
30-40 yrs
>40 yrs
DOI: 10.9790/0853-1411103440
Total no.of cases examined
42
69
46
18
175
Unmarried
31
17
1
49
www.iosrjournals.org
Married
11
52
45
18
126
36 | Page
Clinical Study of Benign Breast Diseases
11
42
< 20yrs
52
69
20-30yrs
45
46
30-40 yrs
18
18
>40
Of the 11 married patients in the age group of <20 yrs, 7 patients were nulliparous and 4 patients were
parous and included 3 lactating mothers. Of the 52 married patients in the age group of 20-30 yrs, 9 patients
were nulliparous and 43 patients were parous and included 7 lactating mothers. Of the 45 married patients in the
age group of 30-40 yrs. 2 patients were nulliparous and 43 patients were parous. All the 18 patients in the age
group >40 yrs, were parous.
Parity distribution of the study group
Age
No.of cases
Unmarried
Nulliparous
Parous
<20 yrs
42
31
20-30 yrs
69
17
43
30-40 yrs
46
43
>40 yrs
18
18
175
49
18
108
Parity distribution of the study
group
80
20-30 yrs
69
70
30-40 yrs
No.of cases
60
50
<20 yrs
>40 yrs
42
46
43 43
40
31
30
18
20
18
17
7 9
10
1 0
2 0
0
No.of cases
Unmarried
Nulliparous
Parous
In this study of 74 cases, 16 cases of 49 unmarried women, 10 cases of the 18 nulliparous women, and
48 cases of the 108 parous women were found to have benign breast diseases.
benign breast diseases
No.of cases
80
74
benign breast diseases
48
60
40
20
10
16
DOI: 10.9790/0853-1411103440
www.iosrjournals.org
37 | Page
Clinical Study of Benign Breast Diseases
No.of cases
As previously mentioned the symptomology with which the women presented to the out patient
department were pain, lump and discharge. The main symptom with which the patient presented was lump. It
was seen 100% of patients with benign breast disease (74 cases). Pain was seen in 56.75% of patients with
benign breast diseases (42 cases). Discharge was seen in 17.56% of patients with benign breast diseases (13
cases).
74
80
70
60
50
40
30
20
10
0
42
No.of cases
13
discharge
pain
lump
Symptoms
Swelling or breast lump was the predominant complaint in fibroadenoma, fibroadenosis, cystosarcoma
Phylloides, and chronic mastitis. Lump associated with pain was seen in fibroadenosis, breast abscess,
tuberculous mastitis, and chronic mastitis.
Pain was the predominant symptom in breast abscess 26% of the patients complaining of pain
(11cases). Pain was more pronounce in breast abscess being continuous and throbbing in nature. Pain of
tuberculous mastitis was also continuous and dull aching in character. Pain of Fibroadenoma and fibroadenosis
was less pronounced and showed variation in relation to the menstrual cycle.
Discharge was seen in 13 patients (17.56%). Discharge was of three types in this study group milky,
serous or pus. The usual discharge was from the nipple. Nipple discharge was milky in breast abscess, serous in
duct ectasia, and pus in breast abscess (milk mixed with pus).
No women in the study group were on oral contraceptive hormonal pills or had used them previously.
None of the women were smokers or alcoholics.
Out of the 14 cases diagnosed clinically as breast abscess initially 12 cases were confirmed on surgery,
and 2 cases were detected to have tuberculous mastitis on surgery and histopathology. Routine pus culture for
microbiology and antibiotic sensitivity; and material of the drained pus for histopathology was not sent in case
of breast abscess. Only for the 2 cases of breast of breast abscesses which showed delayed healing were
scrapings sent for histopatholgical examination on a subsequent day and were diagnosed as being of
tuberculosis. The sensitivity of the clinical examination was 85.7%.
Lactation was found to have a strong association with inflammatory breast diseases; 9 of 11 cases of
breast abscess were lactating (80%), and of the remaining 2 cases of breast abscess 1 women had in abortion 4
weeks before and in 1 case no reason was found. Of the 32 cases diagnosed clinically as Fibroadenoma after
surgery and hisotpathological confirmation 27 cases were actually found to be Fibroadenoma; the sensitivity of
the clinical examination being 84.37%. After hisotpathological examination 3 cases were found to have
fibroadenosis, 1 was found to be a sebaceous cyst and 1 turned to be malignant (Duct cell carcinoma) for which
modified radical mastectomy had to be performed.
Of the 32 cases diagnosed clinically as Fibroadenoma in 25 cases (80%) the lump was seen in the upper
quadrants of the breast. Only in the remaining 7 cases was the lump seen in the lower quadrants. This was
probably due to more breast tissue in the upper quadrants. Bilateral breast involvement was seen only in 1 case
of Fibroadenoma. Multiplicity was not seen.
Of the 23 cases diagnosed clinically as fibroadenosis after surgery and hisotpathological confirmation
20 cases were actually found to be fibroadenosis; the sensitivity of the clinical examination being 86.95%. After
hisotpathological examination 1 case was found to have lipoma and 2 cases were found tuberculous mastitis.
Of the 23 cases diagnosed clinically as fibroadenosis in 19 cases (82.6%) the lump was seen in the
upper quadrants of the breast. Only in the remaining 4 cases was the lump seen in the lower quadrants. Bilateral
breast involvement was seen only in 2 cases fibroadenosis. Multiplicity was not seen.
DOI: 10.9790/0853-1411103440
www.iosrjournals.org
38 | Page
Clinical Study of Benign Breast Diseases
For all the lumps excision / enucleation were performed. For large lumps a corrugated rubber drain was
kept before closing the wound after surgery and removed 24hrs after the surgery. Post operative complications
like hematoma, wound infection were not seen in any cases. But persistence of breast pain even after surgery
and removal of the lump was seen in a few cases for which no reason could be attributed.
In Kings College Hospital Breast Clinic, a study was conducted on breast conditions and 80% of the
patients with breast symptoms were found to have benign breast diseases.
A case control study of benign breast diseases was conducted in Greater Boston in 1968-69.
Fibroadenoma was the commonest benign breast disease and was found during the second decade, mostly seen
in married nullipare. In this study Fibroadenoma was also the most common benign breast making about
43.24% of the cases presented. None of the Fibroadenoma had constant relationship of risk with parity or with
age at first birth in the Boston study. There is however no mention of the significance of tuberculosis in this
study.
Also analysis of black women showed fibrocystic disease as the most frequent disease in both black
and white patients between 25 and 45 yrs of age.
Most western studies have shown that oral contraceptive pills with decreased progesterone reduced risk
of benign breast disease, while a study in the black population revealed no relationship between use of oral
contraceptive pills and incidence of benign breast disease. The use of oral contraceptive pills is extremely low in
the Indian population and the effects of them protective or otherwise cannot be ascertained with certainty. In the
present study none of the women had used oral contraceptive pills.
Most of the Indian studies done are retrospective studies with consequent problems of emphasis. Only
one study by Shukla and Kumar is a prospective study, done in patients with benign breast conditions presenting
at the department of surgery, Varanasi in between 1985-87. 90% of the patients in this study were less than
40yrs. fibroadenosis, Fibroadenoma, tuberculosis, and mastalgia were common in these studies. Also most of
these studies have been done in women in their 40s than in their 20s as subjected to biopsy to rule out the
possibilities of malignant disease in the retrospective.
IV.
Discussion
For correct diagnosis of breast diseases, background knowledge of general features of individual breast
diseases like incidence, age distribution, symptoms
on palpation
findings are very important.
Benignconditions of breast are significantly more common than the malignant conditions in developing
countries. The limited literature available suggests that benign breast disease is a common problem in the
developing countries as well [10]. 74 cases were studied over a period of 28 months. The spectrum of breast
lesions in female patients in our study showed 42.14% benign lesion. Malik [11] in his study of 1724 cases over
a period of 20 years reported benign lesions in 72.97% Similar results,were obtained by Iyer et al. in 2000 [12]
and Mayun et al. in 2008 [13]. In the present study, 55.07% of the benign lesions were noted in the patients
below the age of 25 years. In the same age group, Malik [11] noted benign lesions in 51.19% of the cases and
Bauer [14] in 95% of the cases. The incidence is higher in the study of Bauer [14] as the age group selected for
the study was between 12-22 years. Lump in the breast was the most common presenting symptom in both
benign and malignant groups followed by pain in 10.14% in the benign group and 12.12% in the malignant
group. Dixon et al. [15] conducted a study and found breast lump in 69%, breast pain in 50% and nipple
discharge in 5% of cases. Griffith [16] studied frequency of presenting symptoms in benign breast diseases. He
found common symptoms as lump in 33% of cases followed by pain and nipple discharge and noted that the
patients may present with one or more of the symptoms. In the present study, fibroadenoma was the most
common benign lesion constituting 43.24% followed by fibrocystic disease in 31.08% of the patients. The study
by Malik [11] reported 55% of fibroadenoma. It has been seen that in women between adolescence and the mid
20s, the lobules and the stroma may respond to hormonal stimuli in an exaggerated fashion with the
development of single and multiple fibroadenomas [17]
V.
Conclusions
Benign breast diseases is a common problem in women. A lump in the breast is the commonest
presentation. Breast pain and nipple discharge are the other symptoms. Most of the patients have more than one
symptom. The commonest age group which is affected is the 21-30 years age group. Among the breast lumps,
fibroadenoma is the commonest, followed by fibrocystic changes and breast abscesses. The other lumps are
relatively uncommon. Breast pain may occur alone or in association with a lump or a nipple discharge. The
incidence of cyclical pain is 20% and that of non-cyclical pain is 13%. The nipple discharge, particularly if it is
serous or greenish, is harmless. The clinical diagnoses of the benign breast lumps were accurate in 91.95 %
cases.
The risk factors for developing invasive carcinoma in the patients with proliferative lesions were also
identified and the patients were advised follow-up. Since there is no consensus on the morphologic risk markers,
DOI: 10.9790/0853-1411103440
www.iosrjournals.org
39 | Page
Clinical Study of Benign Breast Diseases
in future, molecular genetic markers may help in the risk stratification, which will help in a better clinical
management.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
[14].
[15].
[16].
[17].
Khemka A, Chakravarti N, Shah S, Patel V. Palpable breast lumps: Fine needle aspiration cytology versus histopathology, a
correlation of diagnostic accuracy. Internet J Surgery. 2009;18:1.
Cole P, Mark Elwood J, Kaplan SD. Incidence rates and risk factors of benign breast neoplasms. Am J Epidemol. 1978;108:11220.
[PubMed]
Hutchinson WB, Thomas DB, Hamlin WB, et al. Risk of breast cancer in women with benign breast lesion. J Natl Cancer Inst.
1980;65:1320. [PubMed]
Kelsey JL, Gammon MD. Epidemiology of breast cancer. Epidemiol Rev. 1990;12:22840. [PubMed]
Sarnelli R, Squartini F. Fibrocystic condition and at risk lesions in asymptomatic breasts, a morphologic study of post menopausal women. Clin Exp. Obstet Gynecol. 1991;18:27179. [PubMed]
Cook MG, Rohan TE. The patho-epidemiology of benign proliferative epithelial disorder of the female breast. J Pathol.
1985;146:115. [PubMed]
Mansel RE. Benign breast disease. Practitioner. 1982;232:83037.
Sainsbury RC. Bailey and Loves Short Practice of Surgery. 25th. London: Edward Arnold Ltd.; 2008. Breast In: Norman WS,
Bulstrode CJK, P.Ronan OConnel editors; pp. 82735.
Love SM, Gelman RS, Silen W. Fibrocystic disease of the breast a non disease? N Eng J Med. 1982;309:101014. [PubMed]
Shukla HS; An outline of benign breast diseases. In Recent advances of surgery, 1992.
Malik R, Bhardwaj VK; Breast lesions in young females. A 20year study forsignificance of early recognition. Indian JPathol
Microbiol., 2003; 46(4): 559-562.
Iyer SP; Epidemiology of Benign BreastDiseases in females of child bearing age group. Bombay Hospital Jr., 2000; 42(1): 141 -146.
Mayun AA, Pindija VH; Pattern of histopathological diagnosis of breast lesion in Gombe, Nigeria. Nigerian J Med., 2008; 17(2):
159-162.
Bauer BS, Jones KM, Talbot CW; Mammary Masses in the advanced females. Surg Gynaecol Obstet., 1987; 165: 3-5.
Dixon JM, Mansel RE; ABC of breast diseases. Symptoms assessment and guidelines for referral. BMJ, 1994; 309(6956):722-726.
Griffith CDM; Benign breast disease. In Sengupta BS, Chattopadhyay SK, Varma TR editors; Gynaecology for post graduates and
practitioners. New Delhi: BI Publications, 1998; 464-475.
Clemons M, Goss P; Estrogens and the risk of breast cancer. N Engl S Med., 2001; 344(4):276-285.
DOI: 10.9790/0853-1411103440
www.iosrjournals.org
40 | Page
Vous aimerez peut-être aussi
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDocument5 pagesAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDocument5 pages"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDocument7 pagesSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDocument4 pagesInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDocument7 pagesA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Document15 pagesA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDocument6 pagesThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Impact of Technologies On Society: A ReviewDocument5 pagesThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- Importance of Mass Media in Communicating Health Messages: An AnalysisDocument6 pagesImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDocument5 pagesEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDocument7 pagesComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDocument5 pagesRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDocument14 pagesAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Assessment of The Implementation of Federal Character in Nigeria.Document5 pagesAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDocument7 pagesTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Lute Against Doping in SportDocument5 pagesThe Lute Against Doping in SportInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Motivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweDocument8 pagesMotivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationDocument6 pagesKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Beowulf: A Folktale and History of Anglo-Saxon Life and CivilizationDocument3 pagesBeowulf: A Folktale and History of Anglo-Saxon Life and CivilizationInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Role of Madarsa Education in Empowerment of Muslims in IndiaDocument6 pagesRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Design Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextDocument6 pagesDesign Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Transforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweDocument9 pagesTransforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Women Empowerment Through Open and Distance Learning in ZimbabweDocument8 pagesWomen Empowerment Through Open and Distance Learning in ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Human Rights and Dalits: Different Strands in The DiscourseDocument5 pagesHuman Rights and Dalits: Different Strands in The DiscourseInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Classical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahDocument9 pagesClassical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- An Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsDocument6 pagesAn Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Micro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaDocument3 pagesMicro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Study On The Television Programmes Popularity Among Chennai Urban WomenDocument7 pagesA Study On The Television Programmes Popularity Among Chennai Urban WomenInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Substance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaDocument11 pagesSubstance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDocument5 pagesDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Breast Cancer Case StudyDocument66 pagesBreast Cancer Case StudyChandan Srivastava100% (2)
- TESTS - Obstetrics and GynecologyDocument38 pagesTESTS - Obstetrics and GynecologyTemitope AdeosunPas encore d'évaluation
- Breast Reviewer (2014)Document7 pagesBreast Reviewer (2014)Jade Monreal0% (1)
- EMLE Trial Exams October 2020 Exams 1000 Q Version (1.0) 9/12/2020Document193 pagesEMLE Trial Exams October 2020 Exams 1000 Q Version (1.0) 9/12/2020Manar AdelPas encore d'évaluation
- Breast - Calcifications Differential Diagnosis: Anatomy Diagnostic ApproachDocument22 pagesBreast - Calcifications Differential Diagnosis: Anatomy Diagnostic ApproachDokdem AjaPas encore d'évaluation
- Iodine RecommendedReadingDocument41 pagesIodine RecommendedReadingproblemcauser100% (2)
- 2011 SLE 1st BankDocument222 pages2011 SLE 1st BankEmad Hajali100% (1)
- Breast Cancer: June 2014Document41 pagesBreast Cancer: June 2014regaPas encore d'évaluation
- Case Study On FCBDDocument38 pagesCase Study On FCBDKwinutskie LiteratoPas encore d'évaluation
- GYNE 9 1 Breast Diseases PDFDocument19 pagesGYNE 9 1 Breast Diseases PDFColeen NeyraPas encore d'évaluation
- Breast Anatomy GuideDocument10 pagesBreast Anatomy GuidessnagaPas encore d'évaluation
- Management of Breast DisordersDocument17 pagesManagement of Breast Disorderskhadzx100% (2)
- Alteration in Reproductive HealthDocument139 pagesAlteration in Reproductive HealthNylia Ollirb AdenipPas encore d'évaluation
- Surgery by HamoudDocument89 pagesSurgery by Hamoudelhamy magdyPas encore d'évaluation
- Breast Imging by DR LinaDocument78 pagesBreast Imging by DR LinahussamPas encore d'évaluation
- Breast CancerDocument129 pagesBreast CancerHope LeePas encore d'évaluation
- Philippine Nursing Assessment Exam ReviewDocument11 pagesPhilippine Nursing Assessment Exam ReviewCzarina Mae Quinones TadeoPas encore d'évaluation
- Matary General Surgery 2013Document309 pagesMatary General Surgery 2013Raouf Ra'fat Soliman100% (8)
- PBL CASE 2 Module 13 Reproductive SystemDocument25 pagesPBL CASE 2 Module 13 Reproductive SystemkaraenPas encore d'évaluation
- Breast Diseases: Detection and Physical ExamDocument22 pagesBreast Diseases: Detection and Physical ExamnicewanPas encore d'évaluation
- Breast Extra Questions 601Document22 pagesBreast Extra Questions 601aminmofrehPas encore d'évaluation
- Case WriteupDocument5 pagesCase WriteupBatool AldaherPas encore d'évaluation
- Breast Pathology Fumc 2022Document145 pagesBreast Pathology Fumc 2022Bahzad AkramPas encore d'évaluation
- The BreastDocument199 pagesThe BreastI.k sidneyPas encore d'évaluation
- Assessment of The BreastDocument11 pagesAssessment of The BreastSIR ONEPas encore d'évaluation
- Pathoma BreastDocument8 pagesPathoma BreastLauren LaMonicaPas encore d'évaluation
- Breast PainDocument8 pagesBreast PainGabriela Zavaleta CamachoPas encore d'évaluation
- Irfan's Shukar BookDocument56 pagesIrfan's Shukar BookHina MalikPas encore d'évaluation
- Breast Cancer Case StudyDocument48 pagesBreast Cancer Case Studyjansestacio93% (54)
- Brest Lump History TakingDocument3 pagesBrest Lump History Takinganon_619577898Pas encore d'évaluation