Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Episode 6: Deductive and Inductive Methods of Teaching: My Learning Episode OverviewDocument10 pagesEpisode 6: Deductive and Inductive Methods of Teaching: My Learning Episode OverviewJustine Elle Vijar85% (13)
- Dafpus 1Document8 pagesDafpus 1Winda WidhyastutiPas encore d'évaluation
- A New Simplified Beading and Boxing Procedure For Elastic ImpressionDocument3 pagesA New Simplified Beading and Boxing Procedure For Elastic ImpressionWinda WidhyastutiPas encore d'évaluation
- Lapsus 1Document3 pagesLapsus 1Winda WidhyastutiPas encore d'évaluation
- Skenario 1 Blok 20 Semester 6 Kelompok 5Document1 pageSkenario 1 Blok 20 Semester 6 Kelompok 5Winda WidhyastutiPas encore d'évaluation
- Tugas Somatitis Gangrenosa Noma (Cancrum Oris)Document1 pageTugas Somatitis Gangrenosa Noma (Cancrum Oris)Winda WidhyastutiPas encore d'évaluation
- Clarifications IntraDocument2 pagesClarifications Intrapm278Pas encore d'évaluation
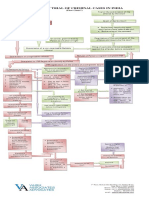
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Bill Vaskis ObitDocument1 pageBill Vaskis ObitSarah TorribioPas encore d'évaluation
- USMLE Step 2 CK Exam - Overview - Examination Content - Test Format - EligibilityDocument7 pagesUSMLE Step 2 CK Exam - Overview - Examination Content - Test Format - EligibilityJamesHowsonPas encore d'évaluation
- English Full Book PaperDocument2 pagesEnglish Full Book PaperSaira BatoolPas encore d'évaluation
- 659.69 BM67 2018-02-06 02 Im Beu-UsaDocument88 pages659.69 BM67 2018-02-06 02 Im Beu-UsaIrakli JibladzePas encore d'évaluation
- Room Air Conditioner: Service ManualDocument68 pagesRoom Air Conditioner: Service Manualervin0% (1)
- Juzaili Alias SSB Jadual Perubahan PDP Dan Penilaian AlternatifDocument1 pageJuzaili Alias SSB Jadual Perubahan PDP Dan Penilaian Alternatifkar afiPas encore d'évaluation
- Mindfulness of Breathing and The Four Elements MeditationDocument98 pagesMindfulness of Breathing and The Four Elements Meditationulrich_ehrenbergerPas encore d'évaluation
- Jee Mathmatic PaperDocument16 pagesJee Mathmatic PaperDeepesh KumarPas encore d'évaluation
- Ingles V Eje 1 Week 2Document5 pagesIngles V Eje 1 Week 2Cristhian Javier Torres PenaPas encore d'évaluation
- Some FactsDocument36 pagesSome Factsapi-281629019Pas encore d'évaluation
- OMCDocument37 pagesOMCyurie_ameliaPas encore d'évaluation
- H.P. Elementary Education Code Chapter - 4 - 2012 SMC by Vijay Kumar HeerDocument7 pagesH.P. Elementary Education Code Chapter - 4 - 2012 SMC by Vijay Kumar HeerVIJAY KUMAR HEERPas encore d'évaluation
- Painter Decorator Curriculum Eng l1 2 3 CC 404c.404dDocument100 pagesPainter Decorator Curriculum Eng l1 2 3 CC 404c.404dM.a. KhaderPas encore d'évaluation
- GO 44 RUDA ExpansionDocument4 pagesGO 44 RUDA ExpansionbharathPas encore d'évaluation
- Swift Case Study Mapping A Path To Iso 20022 With Swift Translator Jan2022Document3 pagesSwift Case Study Mapping A Path To Iso 20022 With Swift Translator Jan2022Bolaji EsanPas encore d'évaluation
- Practical No 4Document5 pagesPractical No 4Mahin SarkarPas encore d'évaluation
- Dragon Is The Fifth in The 12Document3 pagesDragon Is The Fifth in The 12Waylon CahiligPas encore d'évaluation
- SMEC01 CBRS Guide For NBC Reports - v1.1Document53 pagesSMEC01 CBRS Guide For NBC Reports - v1.1phal sovannarithPas encore d'évaluation
- The Honey Gatherers - Travels With The Bauls - The Wandering Minstrels of Rural India - Mimlu Sen PDFDocument16 pagesThe Honey Gatherers - Travels With The Bauls - The Wandering Minstrels of Rural India - Mimlu Sen PDFAurko F AhmadPas encore d'évaluation
- Kanne Gerber Et Al Vineland 2010Document12 pagesKanne Gerber Et Al Vineland 2010Gh8jfyjnPas encore d'évaluation
- Theory of Design 2Document98 pagesTheory of Design 2Thirumeni MadavanPas encore d'évaluation
- Nclex PogiDocument8 pagesNclex Pogijackyd5Pas encore d'évaluation
- Financial Fitness ChecklistDocument4 pagesFinancial Fitness Checklistcoach_22Pas encore d'évaluation
- Question Paper Code:: (10×2 20 Marks)Document2 pagesQuestion Paper Code:: (10×2 20 Marks)Umesh Harihara sudan0% (1)
- Laboratory Manual: Microprocessor & MicrocontrollerDocument4 pagesLaboratory Manual: Microprocessor & Microcontrollershamsul hadiPas encore d'évaluation
- I Am A Filipino by Carlos RomuloDocument7 pagesI Am A Filipino by Carlos RomuloKimberly NgPas encore d'évaluation
- COT Cott Aug 2017Document30 pagesCOT Cott Aug 2017Ala BasterPas encore d'évaluation