Vous aimerez peut-être aussi
- Hodgkin Lymphoma: A Comprehensive OverviewD'EverandHodgkin Lymphoma: A Comprehensive OverviewAndreas EngertPas encore d'évaluation
- Narrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaDocument6 pagesNarrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaJavier Perez ManriquezPas encore d'évaluation
- Atopic Dermatitis: New Perspectives on Managing a Chronic Inflammatory DiseaseD'EverandAtopic Dermatitis: New Perspectives on Managing a Chronic Inflammatory DiseaseÉvaluation : 5 sur 5 étoiles5/5 (1)
- A Preliminary Study To Assess The Efficacy of A New UVA1 Laser For Treatment of PsoriasisDocument5 pagesA Preliminary Study To Assess The Efficacy of A New UVA1 Laser For Treatment of PsoriasisTommaso IannittiPas encore d'évaluation
- Topic 5Document4 pagesTopic 5Rabia BagewadiPas encore d'évaluation
- Ustekinumab TratamentDocument2 pagesUstekinumab Tratamentpanaroxana22Pas encore d'évaluation
- Histologically-Diagnosed Psoriasiform Dermatitis Induced by Nivolumab Successfully Controlled by Etanercept - A Case ReportDocument2 pagesHistologically-Diagnosed Psoriasiform Dermatitis Induced by Nivolumab Successfully Controlled by Etanercept - A Case ReportM CostantinoPas encore d'évaluation
- NB PsoraisisDocument3 pagesNB PsoraisisKhullar VickPas encore d'évaluation
- A Short-Term Trial of Tacrolimus Ointment For Atopic DermatitisDocument6 pagesA Short-Term Trial of Tacrolimus Ointment For Atopic DermatitisRisma WatiPas encore d'évaluation
- A Study of Leprosy Reaction in A Tertiary Hospital in DelhiDocument6 pagesA Study of Leprosy Reaction in A Tertiary Hospital in DelhiamaliaPas encore d'évaluation
- 4 - 2009 Different Applications of MonochromaticDocument8 pages4 - 2009 Different Applications of MonochromaticSandrine SinsoulieuPas encore d'évaluation
- 2009 JDDfinal Acne Isolaz RXDocument3 pages2009 JDDfinal Acne Isolaz RXAndrea MejiaPas encore d'évaluation
- Dihematoporphyrin Ether-Induced Photosensitivity in Laryngeal Papilloma PatientsDocument8 pagesDihematoporphyrin Ether-Induced Photosensitivity in Laryngeal Papilloma PatientsDayse CSMPas encore d'évaluation
- DK CRP B-8 HarmDocument20 pagesDK CRP B-8 HarmCennikon PakpahanPas encore d'évaluation
- Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis Management, Prognosis and Long Term SequelaeDocument28 pagesStevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis Management, Prognosis and Long Term SequelaePutri SRPas encore d'évaluation
- American Journal of Dermatology and Venereology AcneDocument13 pagesAmerican Journal of Dermatology and Venereology AcneErianaSariPas encore d'évaluation
- Treatment of Toxic Epidermal Necrolysis With Intravenous ImmunoglobulinDocument5 pagesTreatment of Toxic Epidermal Necrolysis With Intravenous ImmunoglobulinUbaidillah HafidzPas encore d'évaluation
- The Impact of Stratifying Initial Dose of Corticosteroids by Severity of Pemphigus Vulgaris On Long-Term Disease SeverityDocument6 pagesThe Impact of Stratifying Initial Dose of Corticosteroids by Severity of Pemphigus Vulgaris On Long-Term Disease SeverityArmando LagosPas encore d'évaluation
- Journal of Dermatological ScienceDocument6 pagesJournal of Dermatological ScienceLidwina DewiPas encore d'évaluation
- Brief CommunicationDocument13 pagesBrief CommunicationsantovazPas encore d'évaluation
- PUVA Plus Interferon A2b in The Treatment of Advanced or Refractory To PUVA Early Stage Mycosis Fungoides: A Case SeriesDocument5 pagesPUVA Plus Interferon A2b in The Treatment of Advanced or Refractory To PUVA Early Stage Mycosis Fungoides: A Case Seriesdr.d4Pas encore d'évaluation
- The Effect of Photodynamic Therapy Using Indole-3-Acetic Acid and Green Light On Acne VulgarisDocument5 pagesThe Effect of Photodynamic Therapy Using Indole-3-Acetic Acid and Green Light On Acne VulgarisIqaPas encore d'évaluation
- Research Article: The Effect of Prednisone On Tuberculin Skin Test Reaction in Patients With Rheumatoid ArthritisDocument6 pagesResearch Article: The Effect of Prednisone On Tuberculin Skin Test Reaction in Patients With Rheumatoid ArthritisWidya Ibunda DdffPas encore d'évaluation
- Adverse Cutaneous Drug EruptioDocument13 pagesAdverse Cutaneous Drug EruptioPeroquiePas encore d'évaluation
- Topical Issues in DermatologyDocument8 pagesTopical Issues in DermatologyRohini SelvarajahPas encore d'évaluation
- 3781 FullDocument6 pages3781 FullSukhvinder Singh RanaPas encore d'évaluation
- Jurnal KulitDocument6 pagesJurnal KulitFelicia HalimPas encore d'évaluation
- Skin Treatment With Bepanthen Cream Versus No Cream During Radiotherapy A Randomized Controlled TrialDocument7 pagesSkin Treatment With Bepanthen Cream Versus No Cream During Radiotherapy A Randomized Controlled TrialMaurícioFontanadeVargasPas encore d'évaluation
- Accuracy and UncertaintiesDocument35 pagesAccuracy and UncertaintiesAlvaro Rodrigo Oporto CauzlarichPas encore d'évaluation
- Adverse Cutaneous Drug Eruptions: Current Understanding: ReviewDocument12 pagesAdverse Cutaneous Drug Eruptions: Current Understanding: ReviewasdasdPas encore d'évaluation
- PDF Jurnal PDFDocument6 pagesPDF Jurnal PDFichaPas encore d'évaluation
- Treating Facial Acne in Adolescents and Young Adults With Auriculoacupuncture and AuriculotherapyDocument16 pagesTreating Facial Acne in Adolescents and Young Adults With Auriculoacupuncture and AuriculotherapyPedro MaiaPas encore d'évaluation
- Connective Tissue Diseases: Concepts and Pathogenesis, Overlap Syndromes, Mixed CTD and Undifferentiated CTDDocument9 pagesConnective Tissue Diseases: Concepts and Pathogenesis, Overlap Syndromes, Mixed CTD and Undifferentiated CTDAbuzdea AlexPas encore d'évaluation
- Callen2004 Update On The Management of Cutaneous Lupus ErythematosusDocument6 pagesCallen2004 Update On The Management of Cutaneous Lupus Erythematosusl10n_assPas encore d'évaluation
- Feet Dont Fail Me Anymore Single Centre Results Using Low Dose Radiation Therapy For Feet Inflammatory Disorders and Review of Current EvidenceDocument12 pagesFeet Dont Fail Me Anymore Single Centre Results Using Low Dose Radiation Therapy For Feet Inflammatory Disorders and Review of Current EvidenceAthenaeum Scientific PublishersPas encore d'évaluation
- ClindamycinDocument5 pagesClindamycinDarwyn Paul DagumanPas encore d'évaluation
- Palmoplantar Psoriasis: Treatment With Calcipotriol and Local UVA Radiation Compared With Local PUVADocument5 pagesPalmoplantar Psoriasis: Treatment With Calcipotriol and Local UVA Radiation Compared With Local PUVAFany BijakPas encore d'évaluation
- Local Management of NeutropenicDocument3 pagesLocal Management of NeutropenicCláudia Carrara CotomácioPas encore d'évaluation
- Moretto 2014Document8 pagesMoretto 2014Silvie WidyaPas encore d'évaluation
- Oncotarget 07 59548Document8 pagesOncotarget 07 59548Gustavo DragusPas encore d'évaluation
- Phototherapy FinalDocument86 pagesPhototherapy FinalZunaira ArshadPas encore d'évaluation
- Paper18 25Document8 pagesPaper18 25Rachmat HidayatPas encore d'évaluation
- Topical Application of 1-Methylnicotinamide in The TreatmentDocument4 pagesTopical Application of 1-Methylnicotinamide in The TreatmentHilda FitriaPas encore d'évaluation
- Characterization of Acne Associated With UpadacitiDocument8 pagesCharacterization of Acne Associated With UpadacitiDo u know BTS?Pas encore d'évaluation
- Jurnal BenarDocument4 pagesJurnal BenarSitiMaghfirahHafizPas encore d'évaluation
- Ozone Therapy For Tumor OxygenationDocument11 pagesOzone Therapy For Tumor OxygenationIvan ZuñigaPas encore d'évaluation
- Prenatal X-Ray Exposure and Teratogenic Risks A LiDocument6 pagesPrenatal X-Ray Exposure and Teratogenic Risks A Lidokumentasi kkn81Pas encore d'évaluation
- Nej Mo A 1000067Document13 pagesNej Mo A 1000067Jorg AiPas encore d'évaluation
- Atopic DermatitisDocument6 pagesAtopic DermatitisJhuli Elizabeth CPas encore d'évaluation
- Effectiveness of Low Intensity Laser Therapy On TH PDFDocument5 pagesEffectiveness of Low Intensity Laser Therapy On TH PDFBambang Ulan AeiyuPas encore d'évaluation
- Malignancy Risk and Recurrence With Psoriasis and Its Treatments: A Concise UpdateDocument13 pagesMalignancy Risk and Recurrence With Psoriasis and Its Treatments: A Concise UpdatemogoscristinaPas encore d'évaluation
- JA A D: M CAD ErmatolDocument2 pagesJA A D: M CAD ErmatolIstna Sofia AuliaPas encore d'évaluation
- (OBAT CINA) CAT TherapyDocument6 pages(OBAT CINA) CAT TherapyArga PRPas encore d'évaluation
- ToxicityDocument18 pagesToxicityAbraham OsunaPas encore d'évaluation
- Treatment of Vitiligo With Narrow-Band UVB and Topical Gel Containing Catalase and Superoxide DismutaseDocument5 pagesTreatment of Vitiligo With Narrow-Band UVB and Topical Gel Containing Catalase and Superoxide DismutaseBen IntosiusPas encore d'évaluation
- BTL-6000 High Intensity Laser STUDY Microcirculation EN100 PreviewDocument4 pagesBTL-6000 High Intensity Laser STUDY Microcirculation EN100 PreviewNovaria Puspita SamudraPas encore d'évaluation
- Censabella 2016Document9 pagesCensabella 2016Naiadja Santana CerqueiraPas encore d'évaluation
- Politi Et Al. - 2015 - Integrated Cooling-Vacuum-Assisted 1540-nm ErGlass Laser Is Effective in Treating Mild-To-Moderate AcneDocument5 pagesPoliti Et Al. - 2015 - Integrated Cooling-Vacuum-Assisted 1540-nm ErGlass Laser Is Effective in Treating Mild-To-Moderate AcneNicolás FarkasPas encore d'évaluation
- MDR SleDocument4 pagesMDR SleRamaniya KiranaPas encore d'évaluation
- Recall RadationDocument4 pagesRecall RadationCarolina FernandezPas encore d'évaluation
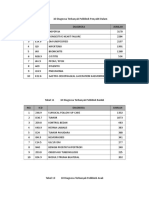
- 10 Diagnosa PenyakitDocument3 pages10 Diagnosa PenyakitDiny Rachma Putri HPas encore d'évaluation
- HBN 6 V1 DssaDocument261 pagesHBN 6 V1 DssaSalsabila Putri UtamiPas encore d'évaluation
- Acute Limb IschemicDocument14 pagesAcute Limb IschemicLuke FloydPas encore d'évaluation
- Superior PDFDocument5 pagesSuperior PDFmhgc108210Pas encore d'évaluation
- School of Law, Galgotias University: Moot PropostionDocument3 pagesSchool of Law, Galgotias University: Moot PropostionwalterPas encore d'évaluation
- Pharmaceutical Biotechnology-QBDocument8 pagesPharmaceutical Biotechnology-QBprateekshaPas encore d'évaluation
- Phlebotomy TechnacianDocument1 pagePhlebotomy Technacianapi-78318377Pas encore d'évaluation
- BotoxMedical Patient BrochureDocument21 pagesBotoxMedical Patient BrochurePatricia Avalos C.Pas encore d'évaluation
- Skin Assessment FormDocument2 pagesSkin Assessment FormOng KarlPas encore d'évaluation
- ?KPSC Assistant Dental Surgeon Exam 2021Document39 pages?KPSC Assistant Dental Surgeon Exam 2021Tejas KulkarniPas encore d'évaluation
- Direction of CureDocument2 pagesDirection of Cureglenn johnstonPas encore d'évaluation
- Thunderbird Medication and Vaccination ProgramDocument1 pageThunderbird Medication and Vaccination ProgramIntsik R. DominadoPas encore d'évaluation
- Patient A (Click On The Link To "Complete Patient A's Karyotype")Document2 pagesPatient A (Click On The Link To "Complete Patient A's Karyotype")ZzaiRraPas encore d'évaluation
- Ob2 Sas 40Document7 pagesOb2 Sas 40????Pas encore d'évaluation
- Group Case Study - Pulmonary TBDocument8 pagesGroup Case Study - Pulmonary TBCj NiñalPas encore d'évaluation
- 358 Muhammad Zul SikkDocument3 pages358 Muhammad Zul SikkMar Yana MamehPas encore d'évaluation
- The Evolving Role of Midwives As Laborists: Original ReviewDocument8 pagesThe Evolving Role of Midwives As Laborists: Original Reviewmnazri98Pas encore d'évaluation
- October 2017 Ophthalmic PearlsDocument3 pagesOctober 2017 Ophthalmic PearlsShafa KhansaPas encore d'évaluation
- Chest Compression Only CPRDocument26 pagesChest Compression Only CPRNicole SorianoPas encore d'évaluation
- English Lesson 1Document7 pagesEnglish Lesson 1In'am TraboulsiPas encore d'évaluation
- Quiz I Categorical Data AnalysisDocument2 pagesQuiz I Categorical Data Analysisfatima fatimaPas encore d'évaluation
- MURMURS - NotespaediaDocument8 pagesMURMURS - NotespaediaZenithPas encore d'évaluation
- NCP 3Document4 pagesNCP 3bananakyuPas encore d'évaluation
- Ma. Cricel T. Dela Cruz, RMTDocument4 pagesMa. Cricel T. Dela Cruz, RMTMa. Cricel T. Dela CruzPas encore d'évaluation
- Sec 5 - Fa - Gas Exchange - T2 - QSDocument3 pagesSec 5 - Fa - Gas Exchange - T2 - QSnoorlailyPas encore d'évaluation
- Nclex PointersDocument4 pagesNclex PointersCarl Michael de Guzman75% (12)
- Organophosphate Poisoning - WikiDocument31 pagesOrganophosphate Poisoning - WikiLIDIYA MOL P VPas encore d'évaluation
- (GPHC) (Autumn) (Closed Book) 2004Document18 pages(GPHC) (Autumn) (Closed Book) 2004aliPas encore d'évaluation
- Structures and Functions of Urinary SystemDocument6 pagesStructures and Functions of Urinary Systemمالك مناصرةPas encore d'évaluation
- Cottenden - Wagg - Supplementary - 23551 ASW Edited Again PDFDocument74 pagesCottenden - Wagg - Supplementary - 23551 ASW Edited Again PDFrohiniPas encore d'évaluation
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (29)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)D'EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Évaluation : 3 sur 5 étoiles3/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (81)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.D'EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Évaluation : 4.5 sur 5 étoiles4.5/5 (110)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessD'EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (328)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceD'EverandTo Explain the World: The Discovery of Modern ScienceÉvaluation : 3.5 sur 5 étoiles3.5/5 (51)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 4 sur 5 étoiles4/5 (5)
- Troubled: A Memoir of Foster Care, Family, and Social ClassD'EverandTroubled: A Memoir of Foster Care, Family, and Social ClassÉvaluation : 4.5 sur 5 étoiles4.5/5 (27)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeD'EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeÉvaluation : 4.5 sur 5 étoiles4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisD'EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 4 sur 5 étoiles4/5 (4)
- The Marshmallow Test: Mastering Self-ControlD'EverandThe Marshmallow Test: Mastering Self-ControlÉvaluation : 4.5 sur 5 étoiles4.5/5 (59)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryD'EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryÉvaluation : 4 sur 5 étoiles4/5 (45)