Vous aimerez peut-être aussi
- When The Going Gets Tough, The Tough Get Going: Social Identification and Individual Effort in Intergroup CompetitionDocument10 pagesWhen The Going Gets Tough, The Tough Get Going: Social Identification and Individual Effort in Intergroup CompetitionLauren Sarah ParkPas encore d'évaluation
- GRE Vocabulary Crossword Puzzle 1Document2 pagesGRE Vocabulary Crossword Puzzle 1Lauren Sarah ParkPas encore d'évaluation
- Abu Lughod Do Muslim Woman Really Need SavingDocument8 pagesAbu Lughod Do Muslim Woman Really Need SavingpatataspanaderaPas encore d'évaluation
- Many Americans Lack Friends of Another RaceDocument2 pagesMany Americans Lack Friends of Another RaceLauren Sarah ParkPas encore d'évaluation
- Bond Lengths and Angles of p-Aminobenzoic AcidDocument1 pageBond Lengths and Angles of p-Aminobenzoic AcidLauren Sarah ParkPas encore d'évaluation
- Guide To MarsDocument119 pagesGuide To MarsLauren Sarah ParkPas encore d'évaluation
- Lauren Park ChemDraw and Spartan - PABADocument1 pageLauren Park ChemDraw and Spartan - PABALauren Sarah ParkPas encore d'évaluation
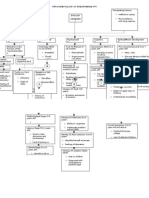
- Flowchart 1Document1 pageFlowchart 1Lauren Sarah ParkPas encore d'évaluation
- Bacterial Growth Experiment Setup and MeasurementDocument1 pageBacterial Growth Experiment Setup and MeasurementLauren Sarah ParkPas encore d'évaluation
- Want To Learn More About The Sangha Metta ProjectDocument2 pagesWant To Learn More About The Sangha Metta ProjectLauren Sarah ParkPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Dissociative Identity DisorderDocument66 pagesDissociative Identity DisorderTemesgen Endalew100% (1)
- Social Anxiety Screening ToolDocument5 pagesSocial Anxiety Screening ToolKurt CutayPas encore d'évaluation
- Bipolar DisorderDocument83 pagesBipolar DisorderEko PriyantoPas encore d'évaluation
- Psychology Disorders Terms Worksheet PDFDocument2 pagesPsychology Disorders Terms Worksheet PDF12345678user100% (1)
- Literature ReviewDocument4 pagesLiterature Reviewapi-548908089Pas encore d'évaluation
- Grace Under Pressure Overcoming Depression 1Document36 pagesGrace Under Pressure Overcoming Depression 1Lordivino T. MesinaPas encore d'évaluation
- My Capstone ProjectDocument25 pagesMy Capstone Projectapi-542755009Pas encore d'évaluation
- Culture SyndromeDocument2 pagesCulture SyndromeNeo AwangPas encore d'évaluation
- The ICD-10 Classification of Mental and Behavioural DisordersDocument263 pagesThe ICD-10 Classification of Mental and Behavioural DisordersMaxim GrossuPas encore d'évaluation
- DeCaluwetal.2014 JClinPsychiatryDocument29 pagesDeCaluwetal.2014 JClinPsychiatryJuan Alberto GonzálezPas encore d'évaluation
- Case Study of ParanoiaDocument2 pagesCase Study of ParanoiaNsengimana Eric MaxigyPas encore d'évaluation
- Schizophrenias: Mental IllnessDocument9 pagesSchizophrenias: Mental IllnessSania AliPas encore d'évaluation
- Neurodevelopmental DisordersDocument26 pagesNeurodevelopmental DisordersJane DoePas encore d'évaluation
- Lock, 2010. Treatment Review Adolescent EDDocument13 pagesLock, 2010. Treatment Review Adolescent EDCarolina GarayPas encore d'évaluation
- A New Empirical Definition of Major Depressive Episode Recovery and Its Positive Impact On Future Course of IllnessDocument19 pagesA New Empirical Definition of Major Depressive Episode Recovery and Its Positive Impact On Future Course of Illnessleeperlhan2000Pas encore d'évaluation
- Psychiatric Case PresentationDocument52 pagesPsychiatric Case PresentationdoreenPas encore d'évaluation
- Scared Child With Scoring 1Document2 pagesScared Child With Scoring 1Fekete OrsolyaPas encore d'évaluation
- What Is Depression?: Depression Is Different From Sadness or Grief/BereavementDocument2 pagesWhat Is Depression?: Depression Is Different From Sadness or Grief/BereavementAdrianaBiabijuxPas encore d'évaluation
- Personality Disorders.: Submitted By: Rhodeliza Mae R. Perhis BS Psychology 3-2Document27 pagesPersonality Disorders.: Submitted By: Rhodeliza Mae R. Perhis BS Psychology 3-2Mark PabalanPas encore d'évaluation
- Journal of Psychiatric Research: SciencedirectDocument7 pagesJournal of Psychiatric Research: SciencedirectAzisahhPas encore d'évaluation
- The Hurricane Movie PaperDocument8 pagesThe Hurricane Movie Paperapi-355282969Pas encore d'évaluation
- Anger, Hostility and AggressionDocument29 pagesAnger, Hostility and AggressionRay Anne Labra-PepitoPas encore d'évaluation
- March Project ProposalDocument2 pagesMarch Project Proposalapi-512175312Pas encore d'évaluation
- Kessler 2005Document11 pagesKessler 2005mccg1478Pas encore d'évaluation
- Psychoeducation: 19 July 2018 Unit VI Topic DiscussionDocument26 pagesPsychoeducation: 19 July 2018 Unit VI Topic DiscussionDana Franklin100% (1)
- 467Document5 pages467Andreea HarhasPas encore d'évaluation
- Mcmi-III - Sample Profile ReportDocument7 pagesMcmi-III - Sample Profile ReportTamara valverde garciaPas encore d'évaluation
- Understanding ADHD in Adults FINALDocument28 pagesUnderstanding ADHD in Adults FINALTyra AtkinsonPas encore d'évaluation
- Michael Alan Taylor, Max Fink-Melancholia - The Diagnosis, Pathophysiology and Treatment of Depressive Illness-Cambridge University Press (2006) PDFDocument561 pagesMichael Alan Taylor, Max Fink-Melancholia - The Diagnosis, Pathophysiology and Treatment of Depressive Illness-Cambridge University Press (2006) PDFPer Sab100% (1)
- Psychopathology Paranoid SchizophreniaDocument2 pagesPsychopathology Paranoid SchizophreniaPrincess Joy T. Catral57% (7)