Vous aimerez peut-être aussi
- The Tai Chi Handbook PDFDocument249 pagesThe Tai Chi Handbook PDFNatasa Zdravkovska100% (5)
- Words For Describing Tone For Writing CommentaryDocument2 pagesWords For Describing Tone For Writing CommentaryDavid ReesePas encore d'évaluation
- The Way of Whips and ChainsDocument31 pagesThe Way of Whips and ChainsRichard Ostrofsky50% (2)
- Osprey Warrior 145 Ottoman Infantryman 1914 18Document68 pagesOsprey Warrior 145 Ottoman Infantryman 1914 18sapiokaravo80% (5)
- Igbo Metaphysics in Chinua AchebeDocument7 pagesIgbo Metaphysics in Chinua AchebeEsùgbamíWilsonÌrosòOgbèPas encore d'évaluation
- How To Contact God Through MeditationDocument7 pagesHow To Contact God Through Meditationmarcelo_vpfPas encore d'évaluation
- An Anti-Racist Approach To Achieving Mental Health Equity in Clinical Care - Legha 2020Document19 pagesAn Anti-Racist Approach To Achieving Mental Health Equity in Clinical Care - Legha 2020EricPas encore d'évaluation
- Kuji-Kiri Technique Overview: Warning: Include (Afftrack - PHP) (Document4 pagesKuji-Kiri Technique Overview: Warning: Include (Afftrack - PHP) (jemleloPas encore d'évaluation
- The Formless Mind EnglishDocument172 pagesThe Formless Mind EnglishManishSavaliaPas encore d'évaluation
- Dua For Students For ConcentrationDocument6 pagesDua For Students For ConcentrationناصرھرەPas encore d'évaluation
- Mouni Sadhu - TheurgyDocument262 pagesMouni Sadhu - TheurgyAMON ADONAI100% (23)
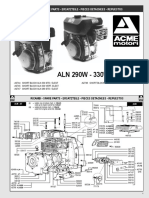
- ACME Engines ALN330WB PDFDocument8 pagesACME Engines ALN330WB PDFsapiokaravo100% (2)
- EpsteinDocument780 pagesEpsteinFatima TrbonjaPas encore d'évaluation
- NWO, Communism & The KahalDocument17 pagesNWO, Communism & The Kahalcuntry_bonerPas encore d'évaluation
- Method of WorshipDocument2 pagesMethod of WorshipyadogopalPas encore d'évaluation
- Human ActsDocument32 pagesHuman ActsBiyaya San Pedro67% (3)
- Altin Kukic - Final Research ReportDocument20 pagesAltin Kukic - Final Research ReportAltin KukicPas encore d'évaluation
- Individual, Provider and System Risk Factor For Breast and Cervical CancerDocument8 pagesIndividual, Provider and System Risk Factor For Breast and Cervical Cancervyvie89Pas encore d'évaluation
- Wiley679ca3db 2eda 20140217073954Document12 pagesWiley679ca3db 2eda 20140217073954Ahmad AbrishamiPas encore d'évaluation
- Jurnal 5Document7 pagesJurnal 5miraPas encore d'évaluation
- Reported Benefits of Participation in A Research StudyDocument6 pagesReported Benefits of Participation in A Research StudyAaron SPas encore d'évaluation
- Maternity MainDocument13 pagesMaternity Mainbayu purnomoPas encore d'évaluation
- Breast Cancer ResearchDocument9 pagesBreast Cancer ResearchSwapnil PatelPas encore d'évaluation
- Minority HealthDocument25 pagesMinority Healthmycatholicvoice.comPas encore d'évaluation
- The Role of Nursing in Cervical Cancer Prevention and TreatmentDocument5 pagesThe Role of Nursing in Cervical Cancer Prevention and TreatmentLytiana WilliamsPas encore d'évaluation
- HLTH 634-d01 Literature ReviewDocument8 pagesHLTH 634-d01 Literature Reviewapi-251046835Pas encore d'évaluation
- Mujer Sana, Familia Fuerte. The Effects of A Culturally - Relevant, Community - Based, Promotores Program To Increase Cervical Cancer Screening Among LatinasDocument13 pagesMujer Sana, Familia Fuerte. The Effects of A Culturally - Relevant, Community - Based, Promotores Program To Increase Cervical Cancer Screening Among LatinasAdrián ÁvilaPas encore d'évaluation
- Effect of Computer Support On Younger Women With Breast CancerDocument11 pagesEffect of Computer Support On Younger Women With Breast CancerAzwar Mustofa WahyudiPas encore d'évaluation
- Vaginal Douching Among LatinasDocument9 pagesVaginal Douching Among LatinasSebastian Posada0% (1)
- HIV Prevalence, Risk Behaviors, Health Care Use, and Mental Health Status of Transgender Persons: Implications For Public Health InterventionDocument7 pagesHIV Prevalence, Risk Behaviors, Health Care Use, and Mental Health Status of Transgender Persons: Implications For Public Health InterventionJuan MoralesPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptYosua_123Pas encore d'évaluation
- Breast Cancer Prevention Knowledge, Attitudes, and Behaviors Among College Women and Mother-Daughter CommunicationDocument10 pagesBreast Cancer Prevention Knowledge, Attitudes, and Behaviors Among College Women and Mother-Daughter CommunicationYuliaPas encore d'évaluation
- NIH Public Access: The Human and Economic Burden of Cervical Cancer in TexasDocument12 pagesNIH Public Access: The Human and Economic Burden of Cervical Cancer in TexassihqinarsrPas encore d'évaluation
- Recovered PDF FileDocument10 pagesRecovered PDF FileAamirPas encore d'évaluation
- Essay 2 Draft 1Document7 pagesEssay 2 Draft 1api-643212890Pas encore d'évaluation
- Using CBPR African Amer Men, Prostate CancerDocument7 pagesUsing CBPR African Amer Men, Prostate CancerpetersonPas encore d'évaluation
- The Import of Trust in Regular Providers To Trust in Cancer Physicians Among White, African American, and Hispanic Breast Cancer PatientsDocument8 pagesThe Import of Trust in Regular Providers To Trust in Cancer Physicians Among White, African American, and Hispanic Breast Cancer PatientsBently JohnsonPas encore d'évaluation
- Best Practice Research Paper FinalDocument11 pagesBest Practice Research Paper Finalapi-354544160Pas encore d'évaluation
- Rectal CancerDocument9 pagesRectal CancerCristina Ștefania RădulescuPas encore d'évaluation
- Gender, Race, Class, and Health: Interrogating The Intersection of Substance Abuse and HIV Through A Cultural LensDocument12 pagesGender, Race, Class, and Health: Interrogating The Intersection of Substance Abuse and HIV Through A Cultural LensMark D SherryPas encore d'évaluation
- Use of Complementary and Alternative Medicine and Breast Cancer Survival in The Health, Eating, Activity, and Lifestyle StudyDocument9 pagesUse of Complementary and Alternative Medicine and Breast Cancer Survival in The Health, Eating, Activity, and Lifestyle StudyIrna SulistiyaniPas encore d'évaluation
- FM MammographyDocument5 pagesFM MammographyAdita DitaPas encore d'évaluation
- Women Offender Transition and Reentry: Gender Responsive Approaches To Transitioning Women Offenders From Prison To The CommunityDocument44 pagesWomen Offender Transition and Reentry: Gender Responsive Approaches To Transitioning Women Offenders From Prison To The CommunityPaola GualterosPas encore d'évaluation
- Authors: Joellen Watson Hawkins: A B B B CDocument4 pagesAuthors: Joellen Watson Hawkins: A B B B Cविजय सिंह धानकPas encore d'évaluation
- Individual PaperDocument9 pagesIndividual Paperapi-354326405Pas encore d'évaluation
- Prostate Cancer and Spirituality - A Systematic ReviewDocument13 pagesProstate Cancer and Spirituality - A Systematic ReviewMarcelo SaadPas encore d'évaluation
- The Inclusion of Women and Minorities in Smoking Cessation Clinical Trials: A Systematic ReviewDocument8 pagesThe Inclusion of Women and Minorities in Smoking Cessation Clinical Trials: A Systematic ReviewJai KunvarPas encore d'évaluation
- Improving Mammography ScreeningDocument8 pagesImproving Mammography ScreeningsylviaramisPas encore d'évaluation
- Variasi Penggunaan Pembersih VaginaDocument13 pagesVariasi Penggunaan Pembersih VaginanovywardanaPas encore d'évaluation
- Huber, Ramnarace McCaffreyDocument6 pagesHuber, Ramnarace McCaffreyAna MoraisPas encore d'évaluation
- Fielding Miller2020Document13 pagesFielding Miller2020ucan fajrinPas encore d'évaluation
- 1-s2.0-S1054139X16307352-main Intimate Partner ViolenceDocument2 pages1-s2.0-S1054139X16307352-main Intimate Partner ViolenceVissente TapiaPas encore d'évaluation
- World Journal of Surgical OncologyDocument9 pagesWorld Journal of Surgical OncologyNikita BowmanPas encore d'évaluation
- Intimate Partner Violence and Cancer Screening Among Urban Minority WomenDocument11 pagesIntimate Partner Violence and Cancer Screening Among Urban Minority WomenLauraPalmerPas encore d'évaluation
- Singer, Judy Qualitative Evaluation of A Community NavajoDocument15 pagesSinger, Judy Qualitative Evaluation of A Community NavajoLuis R HdezPas encore d'évaluation
- 2022 Article 1107Document8 pages2022 Article 1107Armando NogueraPas encore d'évaluation
- Essay 2 Draft 1 1Document7 pagesEssay 2 Draft 1 1api-643212890Pas encore d'évaluation
- The Lancet Sobre A Saúde Das Pessoas TransDocument25 pagesThe Lancet Sobre A Saúde Das Pessoas TransgeorgeenfPas encore d'évaluation
- The Effects of Cancer Survivorship On Families and CaregiversDocument6 pagesThe Effects of Cancer Survivorship On Families and CaregiversNurul ShahirahPas encore d'évaluation
- Research Paper Womens HealthDocument7 pagesResearch Paper Womens Healthhxmchprhf100% (1)
- Hispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research LiteratureDocument27 pagesHispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research LiteratureUrbanYouthJusticePas encore d'évaluation
- Evaluating Treatment Experiences Among Peer MentorsD'EverandEvaluating Treatment Experiences Among Peer MentorsPas encore d'évaluation
- Academic Policy Advisor: Health Policy and ManagementDocument7 pagesAcademic Policy Advisor: Health Policy and Managementchar2183Pas encore d'évaluation
- JPM Hebert 2009Document10 pagesJPM Hebert 2009Oana RusuPas encore d'évaluation
- J SXMR 2016 02 006Document6 pagesJ SXMR 2016 02 006nmiratPas encore d'évaluation
- Hispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research Literature Prepared by Luis H. Zayas, Ph.D.Document2 pagesHispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research Literature Prepared by Luis H. Zayas, Ph.D.UrbanYouthJusticePas encore d'évaluation
- Research On CancerDocument11 pagesResearch On Cancerrubyshah886Pas encore d'évaluation
- BMC Health Services Research: Digging Deeper: Quality of Patient-Provider Communication Across Hispanic SubgroupsDocument8 pagesBMC Health Services Research: Digging Deeper: Quality of Patient-Provider Communication Across Hispanic SubgroupsTitan LinggastiwiPas encore d'évaluation
- Mental Health of Sexual MinoritiesDocument12 pagesMental Health of Sexual MinoritiesjoePas encore d'évaluation
- RSM Article Assignment (A - 3)Document3 pagesRSM Article Assignment (A - 3)Zara KhanPas encore d'évaluation
- Running Head: Health Teaching Plan For Breast Cancer PreventionDocument9 pagesRunning Head: Health Teaching Plan For Breast Cancer PreventionAnthony LopezPas encore d'évaluation
- The Power and The Promise Working With Communities - Cashman Israel Et Al 2008 3Document12 pagesThe Power and The Promise Working With Communities - Cashman Israel Et Al 2008 3api-232023635Pas encore d'évaluation
- Chapter 1 EditedDocument8 pagesChapter 1 Editedroneldayo62Pas encore d'évaluation
- LKJMNDocument11 pagesLKJMNCatur AndrianPas encore d'évaluation
- Transplanting Care: Shifting Commitments in Health and Care in the United StatesD'EverandTransplanting Care: Shifting Commitments in Health and Care in the United StatesPas encore d'évaluation
- 1896Document76 pages1896sapiokaravoPas encore d'évaluation
- Growing MagnoliasDocument3 pagesGrowing MagnoliassapiokaravoPas encore d'évaluation
- What Reasonably Expect?: The Contribution of School Health Education Community Health Promotion: CanDocument8 pagesWhat Reasonably Expect?: The Contribution of School Health Education Community Health Promotion: CansapiokaravoPas encore d'évaluation
- Works? A Literature Review. Preventing Childhood Unintentional Injuries - WhatDocument11 pagesWorks? A Literature Review. Preventing Childhood Unintentional Injuries - WhatsapiokaravoPas encore d'évaluation
- Dharma Bharathi New Age in Catholic Educational InstitutionsDocument79 pagesDharma Bharathi New Age in Catholic Educational InstitutionsFrancis LoboPas encore d'évaluation
- PerfectionismDocument87 pagesPerfectionismPaul Jorge TaglePas encore d'évaluation
- Testimonials For James W Jesso Nov 2013Document3 pagesTestimonials For James W Jesso Nov 2013James W. JessoPas encore d'évaluation
- Studying The Quran in The Muslim Academy Majid Daneshgar Full Chapter PDF ScribdDocument67 pagesStudying The Quran in The Muslim Academy Majid Daneshgar Full Chapter PDF Scribdleslie.dedeke821100% (6)
- The Call To MinistryDocument3 pagesThe Call To MinistryAnonymous JluiZrw6Pas encore d'évaluation
- History ProjectDocument18 pagesHistory Projectaayush choudharyPas encore d'évaluation
- Su 'Per La Verità', Di Diego Marconi PDFDocument19 pagesSu 'Per La Verità', Di Diego Marconi PDFMarisa La BarberaPas encore d'évaluation
- False Prophets of The Watchtower PDFDocument203 pagesFalse Prophets of The Watchtower PDFnicodemof71100% (2)
- SpurgeonPreaching PDFDocument5 pagesSpurgeonPreaching PDFsujithsamuelPas encore d'évaluation
- Jamia Masjid Behzad Lakhnavi and Madrassa: Subject Name: Teacher's NameDocument14 pagesJamia Masjid Behzad Lakhnavi and Madrassa: Subject Name: Teacher's Namebaap playerPas encore d'évaluation
- A History of PolandDocument3 pagesA History of Polandvidur_talrejaPas encore d'évaluation
- Introduction To Philosophical Methods PDFDocument17 pagesIntroduction To Philosophical Methods PDFAnand Kumar YadavPas encore d'évaluation
- Rishi Dadhichi PDFDocument2 pagesRishi Dadhichi PDFNilkanth YengdePas encore d'évaluation
- Title: Implementation of Campus Ministry Activities: Implication To Quality SpiritualDocument7 pagesTitle: Implementation of Campus Ministry Activities: Implication To Quality SpiritualFORCHIA MAE CUTARPas encore d'évaluation
- AuditorList For Class ADocument49 pagesAuditorList For Class Ajena filingPas encore d'évaluation
- EQ040108 NashDocument16 pagesEQ040108 NashAnonymous 77zvHWsPas encore d'évaluation
- Summer 2013 NewsletterDocument6 pagesSummer 2013 NewsletterTibetan Canadian Cultural CentrePas encore d'évaluation