Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Keogh ComplaintDocument5 pagesKeogh ComplaintWIS Digital News StaffPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- B325 MTA 2017-2018- ساره هلال الخالدي- second courseDocument14 pagesB325 MTA 2017-2018- ساره هلال الخالدي- second courseAmethyst Online67% (3)
- ASSIGNMENT - Employment and Industrial LawDocument18 pagesASSIGNMENT - Employment and Industrial LawAhmad Hirzi Azni50% (2)
- Not Economics But Politics - OutlineDocument3 pagesNot Economics But Politics - OutlineSheikh Abdul Wahab0% (1)
- Atlantic Council and Burisma Sign Cooperation AgreementDocument3 pagesAtlantic Council and Burisma Sign Cooperation AgreementDSU Deep State UnveiledPas encore d'évaluation
- Classical School of ThoughtDocument5 pagesClassical School of ThoughtJannus AmarillePas encore d'évaluation
- David Attwell's Tribute To Nelson MandelaDocument3 pagesDavid Attwell's Tribute To Nelson MandelaSA BooksPas encore d'évaluation
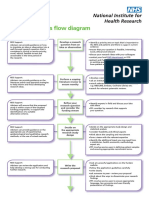
- Research Process Flow Chart A4 WebDocument2 pagesResearch Process Flow Chart A4 WebEma FatimahPas encore d'évaluation
- Further White Estate Lawsuit Negotiation CorrespondenceDocument16 pagesFurther White Estate Lawsuit Negotiation CorrespondenceDanielBabylone100% (1)
- 11th Lecture Deen and ShariahDocument24 pages11th Lecture Deen and ShariahMariam RiazPas encore d'évaluation
- Cyber Bullying ScriptDocument3 pagesCyber Bullying ScriptMonica Eguillion100% (1)
- A Psychological Study of Nathaniel Hawthorne'S The: Scarlet LatterDocument10 pagesA Psychological Study of Nathaniel Hawthorne'S The: Scarlet LatterRomilyn PiocPas encore d'évaluation
- Admin Case DigestsDocument50 pagesAdmin Case DigestsJennyMariedeLeon100% (1)
- 0648 ThinkPeopleFirst Dds 08222014Document2 pages0648 ThinkPeopleFirst Dds 08222014Vaishnavi JayakumarPas encore d'évaluation
- The Roots of The Filipino People: The EpilogueDocument16 pagesThe Roots of The Filipino People: The EpilogueSteve B. Salonga100% (1)
- Language Revision, A WorksheetDocument4 pagesLanguage Revision, A WorksheetJaime MontoyaPas encore d'évaluation
- The Politics of Transition in Kenya: From KANU To NARC, 2003Document217 pagesThe Politics of Transition in Kenya: From KANU To NARC, 2003jakarta100% (6)
- Cirtical Thinking Review Questions Mr. IsmaelDocument8 pagesCirtical Thinking Review Questions Mr. IsmaelKura .DlshkawPas encore d'évaluation
- Contract PMS ServiceDocument3 pagesContract PMS ServiceCalvin Patrick DomingoPas encore d'évaluation
- Vwca AgreementDocument51 pagesVwca Agreementworkcovervictim8242Pas encore d'évaluation
- Noting: Definition of NoteDocument5 pagesNoting: Definition of NoteNehaPas encore d'évaluation
- 3.0.0 FSO 13 DimensionsDocument1 page3.0.0 FSO 13 DimensionsRose LeePas encore d'évaluation
- CodicilDocument2 pagesCodicilJJ Gapol100% (4)
- A Poem For Cotton PickersDocument4 pagesA Poem For Cotton Pickersapi-447987846Pas encore d'évaluation
- Internship Report NgoDocument14 pagesInternship Report Ngosamarth chauhanPas encore d'évaluation
- What Is Your Philosophy in LifeDocument3 pagesWhat Is Your Philosophy in LifeArvin EleuterioPas encore d'évaluation
- Melody Gardot Your Heart Is As Black As NightDocument8 pagesMelody Gardot Your Heart Is As Black As NightmiruPas encore d'évaluation
- G.R. Nos. L-27425 & L-30505 - Converse Rubber Vs Jacinto RubberDocument8 pagesG.R. Nos. L-27425 & L-30505 - Converse Rubber Vs Jacinto RubberArmand Patiño AlforquePas encore d'évaluation
- Position PaperDocument9 pagesPosition PaperJamellen De Leon BenguetPas encore d'évaluation
- PD 603 - Child and Youth Welfare CodeDocument9 pagesPD 603 - Child and Youth Welfare CodeJhon RamirezPas encore d'évaluation