Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- CA Hepar RadiologiDocument18 pagesCA Hepar RadiologiMarcellRaymondPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Ruptur PerineumDocument7 pagesRuptur PerineumMarcellRaymondPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Immunological Mechanisms in Allergic Contact Dermatitis: Abstract and IntroductionDocument11 pagesImmunological Mechanisms in Allergic Contact Dermatitis: Abstract and IntroductionMarcellRaymondPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Cardiovascular Emergency..Document120 pagesCardiovascular Emergency..MarcellRaymondPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Rupture PerineumDocument26 pagesRupture PerineumMarcellRaymondPas encore d'évaluation
- Pulmonary DisordersDocument53 pagesPulmonary DisordersAhmad Makhlouf100% (1)
- College of Health Sciences: Urdaneta City UniversityDocument3 pagesCollege of Health Sciences: Urdaneta City UniversityJorgie CastroPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Asrs Common Retina CPT CodesDocument3 pagesAsrs Common Retina CPT Codesapi-405859281Pas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Intradermal Injection PDFDocument2 pagesIntradermal Injection PDFSean Philippe CabralPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Pharmaceutical Equivalence of Generic Essential DrugsDocument15 pagesPharmaceutical Equivalence of Generic Essential DrugsLiiz PinedaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Usmani 2021 AerosphereDocument12 pagesUsmani 2021 AerosphereRadu CiprianPas encore d'évaluation
- ZyprexaDocument5 pagesZyprexaSuzetteBragaSamuelaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
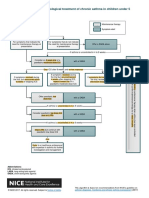
- Algorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5Document1 pageAlgorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5samPas encore d'évaluation
- Triamcinolone Clinical - PREA PDFDocument62 pagesTriamcinolone Clinical - PREA PDFnephylymPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Mylan Vs Biogen '514 Tecfidera IPR InstitutionDocument47 pagesMylan Vs Biogen '514 Tecfidera IPR InstitutionTradeHawkPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- New Guide To Medicines & Drugs - K TORODocument514 pagesNew Guide To Medicines & Drugs - K TOROKreshnik Idrizaj100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Botox Blocks Buzzers Migraine in Kids 4-22-23Document14 pagesBotox Blocks Buzzers Migraine in Kids 4-22-23Jere AyerbePas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Drug Development and Delivery - March 2011Document77 pagesDrug Development and Delivery - March 2011Gustavo FuchsPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Onato Sami PharmaDocument1 pageOnato Sami PharmaNabeel Ahmed KhanPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Cmhs T.timetable For Year 3 4 5-Trim.2 3 F. Draft - Huye CDocument90 pagesCmhs T.timetable For Year 3 4 5-Trim.2 3 F. Draft - Huye CAurelius Jean de DieuPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Coumadin WarfarinDocument1 pageCoumadin WarfarinSheri490100% (1)
- Clinical Practice Guidelines in Antibiotic Prophylaxis in ElectiveDocument52 pagesClinical Practice Guidelines in Antibiotic Prophylaxis in ElectiveNikekier Perez100% (1)
- TrazodoneDocument20 pagesTrazodoneAjay MehtaPas encore d'évaluation
- Formulative Pharmacy and BiopharmaceuticsDocument16 pagesFormulative Pharmacy and BiopharmaceuticsJafrine100% (1)
- MD Pharmacology Question Papers 2019-06-17 11.48.23Document11 pagesMD Pharmacology Question Papers 2019-06-17 11.48.23Vijendra R100% (1)
- Drug StudyDocument1 pageDrug StudyBSN 3-2 RUIZ, Jewel Anne F.Pas encore d'évaluation
- Bisoprolol PDFDocument69 pagesBisoprolol PDFDuwi Efasari100% (3)
- Procedure TraysDocument4 pagesProcedure TraysAnusha VerghesePas encore d'évaluation
- QCPP Requirements ManualDocument241 pagesQCPP Requirements Manualron220% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- v10 Treatment of Viral Warts With Intralesional BleomycinDocument5 pagesv10 Treatment of Viral Warts With Intralesional BleomycinAlisPas encore d'évaluation
- Routes of Drug AdministrationDocument24 pagesRoutes of Drug Administrationmftaganas100% (1)
- Drug Interactions of Veterinary Importance With Reference To Fluid TherapyDocument29 pagesDrug Interactions of Veterinary Importance With Reference To Fluid TherapySunil67% (3)
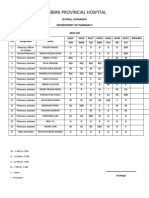
- Lumbini Provincial Hospital: Department of PharmacyDocument2 pagesLumbini Provincial Hospital: Department of PharmacyImdadHussainOPositivePas encore d'évaluation
- Adverse Reactions SlideshowDocument40 pagesAdverse Reactions SlideshowGary MaoPas encore d'évaluation
- Laporan Supernova Wiji - AgustusDocument5 pagesLaporan Supernova Wiji - Agustusrahma dewi styaningrumPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)