Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Musical Theatre Audition SuggestionsDocument3 pagesMusical Theatre Audition SuggestionsMarjun Valdez100% (8)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Foundation of Special & Inclusive EducationDocument15 pagesFoundation of Special & Inclusive Educationnina soPas encore d'évaluation
- Dave Mearns - Person-Centred Counselling Training-SAGE (1997)Document247 pagesDave Mearns - Person-Centred Counselling Training-SAGE (1997)dd1335100% (4)
- ProgramDocument2 pagesProgramapi-25919517100% (1)
- Pinggang PinoyDocument9 pagesPinggang Pinoyjreyab100% (1)
- Legalization of EuthanasiaDocument9 pagesLegalization of EuthanasiaDaniel Sabori HerreraPas encore d'évaluation
- Problem Set 1Document1 pageProblem Set 1Timothy WilliamsPas encore d'évaluation
- Transmission Genetics: Genetics Analysis: An Integrated ApproachDocument52 pagesTransmission Genetics: Genetics Analysis: An Integrated ApproachTimothy WilliamsPas encore d'évaluation
- Genetics Review Guide Ch 2-13, 21-22Document4 pagesGenetics Review Guide Ch 2-13, 21-22Timothy WilliamsPas encore d'évaluation
- Probability Calculations in Genetics Problem Solving: Genetics Analysis: An Integrated ApproachDocument44 pagesProbability Calculations in Genetics Problem Solving: Genetics Analysis: An Integrated ApproachTimothy WilliamsPas encore d'évaluation
- 15 Green Chartreuse-B - Clarinet - IIDocument1 page15 Green Chartreuse-B - Clarinet - IITimothy WilliamsPas encore d'évaluation
- 16 Your Little Lover - FluteDocument2 pages16 Your Little Lover - FluteTimothy WilliamsPas encore d'évaluation
- 15 Green Chartreuse-OboeDocument1 page15 Green Chartreuse-OboeTimothy WilliamsPas encore d'évaluation
- 5 Green Chartreuse-BassoonDocument1 page5 Green Chartreuse-BassoonTimothy WilliamsPas encore d'évaluation
- L'Etoile - 17 Couplet of The Rose-A - Clarinet - IDocument1 pageL'Etoile - 17 Couplet of The Rose-A - Clarinet - ITimothy WilliamsPas encore d'évaluation
- 16 Your Little Lover - A - Clarinet - IIDocument1 page16 Your Little Lover - A - Clarinet - IITimothy WilliamsPas encore d'évaluation
- 15 Green Chartreuse-PiccoloDocument1 page15 Green Chartreuse-PiccoloTimothy WilliamsPas encore d'évaluation
- L'Etoile - 17 Couplet of The Rose-Bassoon PDFDocument1 pageL'Etoile - 17 Couplet of The Rose-Bassoon PDFTimothy WilliamsPas encore d'évaluation
- 17 Couplet of The Rose-BassoonDocument1 page17 Couplet of The Rose-BassoonTimothy WilliamsPas encore d'évaluation
- 16 Your Little Lover - OboeDocument1 page16 Your Little Lover - OboeTimothy WilliamsPas encore d'évaluation
- 17 Couplet of The Rose-A - Clarinet - IIDocument1 page17 Couplet of The Rose-A - Clarinet - IITimothy WilliamsPas encore d'évaluation
- 6 Act One Finale-Cymbal, - Bass - Drum, - TriangleDocument3 pages6 Act One Finale-Cymbal, - Bass - Drum, - TriangleTimothy WilliamsPas encore d'évaluation
- L'Etoile - 17 Couplet of The Rose-Flute PDFDocument1 pageL'Etoile - 17 Couplet of The Rose-Flute PDFTimothy WilliamsPas encore d'évaluation
- 18 Burgomaster - BassoonDocument1 page18 Burgomaster - BassoonTimothy WilliamsPas encore d'évaluation
- 17 Couplet of The Rose-OboeDocument1 page17 Couplet of The Rose-OboeTimothy WilliamsPas encore d'évaluation
- 17 Couplet of The Rose-FluteDocument1 page17 Couplet of The Rose-FluteTimothy WilliamsPas encore d'évaluation
- 7 Drinking Song-PercussionDocument2 pages7 Drinking Song-PercussionTimothy WilliamsPas encore d'évaluation
- 5 Trio and Tickling Couplets-Timpani - GlockenspielDocument2 pages5 Trio and Tickling Couplets-Timpani - GlockenspielTimothy WilliamsPas encore d'évaluation
- 18 Burgomaster - A - Clarinet - IDocument1 page18 Burgomaster - A - Clarinet - ITimothy WilliamsPas encore d'évaluation
- 18a Funeral-FluteDocument1 page18a Funeral-FluteTimothy WilliamsPas encore d'évaluation
- L'Etoile - 18a Funeral-B - Clarinet - IIDocument1 pageL'Etoile - 18a Funeral-B - Clarinet - IITimothy WilliamsPas encore d'évaluation
- 18a Funeral-BassoonDocument1 page18a Funeral-BassoonTimothy WilliamsPas encore d'évaluation
- 7 Drinking Song-Violin - IDocument3 pages7 Drinking Song-Violin - ITimothy WilliamsPas encore d'évaluation
- Fainting Quartet-Violin - IDocument1 pageFainting Quartet-Violin - ITimothy WilliamsPas encore d'évaluation
- Fainting Quartet-Violin - IIDocument1 pageFainting Quartet-Violin - IITimothy WilliamsPas encore d'évaluation
- Mario and Bowsette in The Blazes of Love - ComicsNixDocument1 pageMario and Bowsette in The Blazes of Love - ComicsNixBryan DiazPas encore d'évaluation
- Available BoneDocument46 pagesAvailable BoneAkanksha MahajanPas encore d'évaluation
- Full Test Bank For Introduction To Health Care Finance and Accounting 1St Edition Carlene Harrison William P Harrison PDF Docx Full Chapter ChapterDocument36 pagesFull Test Bank For Introduction To Health Care Finance and Accounting 1St Edition Carlene Harrison William P Harrison PDF Docx Full Chapter Chaptercitiedcorneuleb4ket100% (8)
- Final Manuscript of Group 1Document104 pagesFinal Manuscript of Group 1AYLEYA L. MAGDAONGPas encore d'évaluation
- SI (Main) 11 30Document57 pagesSI (Main) 11 30Zainab KhanPas encore d'évaluation
- Stok OpnameDocument19 pagesStok OpnameeniPas encore d'évaluation
- Clinical review of skin scarring diagnosis and treatmentDocument5 pagesClinical review of skin scarring diagnosis and treatmentjoshuaPas encore d'évaluation
- Health EssayDocument2 pagesHealth EssaykieraPas encore d'évaluation
- Placemaking As An Approach of Sustainable Urban Facilities ManagementDocument2 pagesPlacemaking As An Approach of Sustainable Urban Facilities ManagementKeziahjan ValenzuelaPas encore d'évaluation
- Performence Appraisal For PracticeDocument18 pagesPerformence Appraisal For PracticeAnusha VerghesePas encore d'évaluation
- Presented By: 1) S.Chandra Prakash 2) Rohith Sirpa Iii B.Tech Bme, BvritDocument21 pagesPresented By: 1) S.Chandra Prakash 2) Rohith Sirpa Iii B.Tech Bme, BvritBiplav EvolvesPas encore d'évaluation
- Benefits of JCI and ISO AccreditationDocument7 pagesBenefits of JCI and ISO AccreditationOdesa AvilesPas encore d'évaluation
- Paper PE Rabies Bali - Chaerul BasriDocument14 pagesPaper PE Rabies Bali - Chaerul BasriAulia Miftakhur RahmanPas encore d'évaluation
- Occupational Therapy For MNDDocument92 pagesOccupational Therapy For MNDSharifPas encore d'évaluation
- TINFC-2020-03 paragraph structure practiceDocument3 pagesTINFC-2020-03 paragraph structure practiceMuchamad SolehPas encore d'évaluation
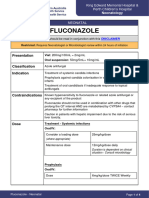
- FluconazoleDocument4 pagesFluconazoleeucaPas encore d'évaluation
- Feeding ProgramDocument20 pagesFeeding ProgramAnalyn DominguezPas encore d'évaluation
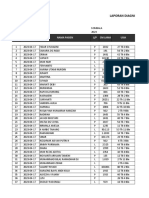
- Laporan Diagnosa Pasien Harian: Puskesmas: TanggalDocument9 pagesLaporan Diagnosa Pasien Harian: Puskesmas: TanggalRamlawatiPas encore d'évaluation
- UGIHDocument59 pagesUGIHEkkawit IamthonginPas encore d'évaluation
- Introduction to Family Health: Roles, Functions, and DeterminantsDocument29 pagesIntroduction to Family Health: Roles, Functions, and DeterminantsMuktarPas encore d'évaluation
- MOV - 1.2 Attendance Sheet For Social Mobilization-1Document2 pagesMOV - 1.2 Attendance Sheet For Social Mobilization-1PHO KALINGAPas encore d'évaluation
- Model Edukasi Postnatal Melalui Pendekatan FamilyDocument19 pagesModel Edukasi Postnatal Melalui Pendekatan FamilyAgustina VivoPas encore d'évaluation
- ALLTEST Quotation Sheet-Globiome Society-Maimouna-Senegal-20231016Document2 pagesALLTEST Quotation Sheet-Globiome Society-Maimouna-Senegal-20231016globiomePas encore d'évaluation
- TFN Finals ReviewerDocument3 pagesTFN Finals Reviewerediyette parduaPas encore d'évaluation
- Electrical Safety Signs ExplainedDocument38 pagesElectrical Safety Signs ExplainedNarfred EgarPas encore d'évaluation