Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Diabetes CPG Training ModuleDocument158 pagesDiabetes CPG Training Modulenirmalkumaar88Pas encore d'évaluation
- Clinical Practice Guidelines: Management of Type 2 Diabetes MellitusDocument33 pagesClinical Practice Guidelines: Management of Type 2 Diabetes Mellitusnirmalkumaar88100% (1)
- Clinical Practice Guidelines: Management of Type 2 Diabetes MellitusDocument6 pagesClinical Practice Guidelines: Management of Type 2 Diabetes Mellitusnirmalkumaar88Pas encore d'évaluation
- Clinical Practice Guidelines: Management of Type 2 Diabetes MellitusDocument20 pagesClinical Practice Guidelines: Management of Type 2 Diabetes Mellitusnirmalkumaar88Pas encore d'évaluation
- 01 Overview of Diabetes CPGDocument15 pages01 Overview of Diabetes CPGnirmalkumaar88Pas encore d'évaluation
- Award 14085Document21 pagesAward 14085nirmalkumaar88Pas encore d'évaluation
- Traxxfm Election ReleaseDocument3 pagesTraxxfm Election Releasenirmalkumaar88Pas encore d'évaluation
- HW ChemistryDocument1 pageHW Chemistrynirmalkumaar88Pas encore d'évaluation
- Bank Copy Depositor Copy Nirmal Darbar Copy: Axis Bank Axis Bank Axis BankDocument1 pageBank Copy Depositor Copy Nirmal Darbar Copy: Axis Bank Axis Bank Axis Banknirmalkumaar88Pas encore d'évaluation
- McDonald Marissa - Dysphoric Milk Ejection ReflexDocument14 pagesMcDonald Marissa - Dysphoric Milk Ejection Reflexnirmalkumaar88Pas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Internet Addiction Kids and The South Korean Govt Boot CampsDocument5 pagesInternet Addiction Kids and The South Korean Govt Boot Campslgheorma0Pas encore d'évaluation
- Zotc 116 Exer 3Document2 pagesZotc 116 Exer 3Leighna Ricci CruzPas encore d'évaluation
- Form 1 ADocument2 pagesForm 1 ARohit Jain100% (2)
- Free End SaddleDocument5 pagesFree End SaddleAdry AnnaPas encore d'évaluation
- Understanding My Benefits: Pre - Auth@Document2 pagesUnderstanding My Benefits: Pre - Auth@Jonelle Morris-DawkinsPas encore d'évaluation
- Risk Assessment - Lifting OperationsDocument6 pagesRisk Assessment - Lifting OperationsJishad Nalakath83% (87)
- DebateDocument12 pagesDebate•Kai yiii•Pas encore d'évaluation
- HHHHHGGGDocument7 pagesHHHHHGGGemrangiftPas encore d'évaluation
- Introduction To Different Resources of Bioinformatics and Application PDFDocument55 pagesIntroduction To Different Resources of Bioinformatics and Application PDFSir RutherfordPas encore d'évaluation
- New Yorkers in Need Poverty TrendsDocument44 pagesNew Yorkers in Need Poverty Trendsshughes080Pas encore d'évaluation
- 5.3.1 Distinguish Between Learning and Performance: Skill in SportDocument48 pages5.3.1 Distinguish Between Learning and Performance: Skill in SportAiham AltayehPas encore d'évaluation
- Checking Vital SighnDocument14 pagesChecking Vital SighnAdimas AnggaraPas encore d'évaluation
- HLSC 641 AT3 Critical AppraisalDocument24 pagesHLSC 641 AT3 Critical AppraisalAnastasia Eghogho OkohPas encore d'évaluation
- Drug Study - MidazolamDocument8 pagesDrug Study - MidazolamKian HerreraPas encore d'évaluation
- Climbing Training Log - TemplateDocument19 pagesClimbing Training Log - TemplateKam Iqar ZePas encore d'évaluation
- Neurobiologic Theories and PsychopharmacologyDocument2 pagesNeurobiologic Theories and Psychopharmacologymyer pasandalanPas encore d'évaluation
- Optical DXH 800Document1 pageOptical DXH 800Gregorio De Las CasasPas encore d'évaluation
- Platelet Analysis - An Overview: HistoryDocument7 pagesPlatelet Analysis - An Overview: HistoryPieter Du Toit-EnslinPas encore d'évaluation
- Pacific CrossDocument27 pagesPacific Crossanon_873405382Pas encore d'évaluation
- DR John Chew (SPMPS President) PresentationDocument50 pagesDR John Chew (SPMPS President) PresentationdrtshPas encore d'évaluation
- What Is FOCUS CHARTINGDocument38 pagesWhat Is FOCUS CHARTINGSwen Digdigan-Ege100% (2)
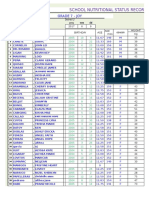
- School Nutritional Status Record: Grade 7 - JoyDocument4 pagesSchool Nutritional Status Record: Grade 7 - JoySidPas encore d'évaluation
- Redfern Mianscum LetterDocument6 pagesRedfern Mianscum LettermediaindigenaPas encore d'évaluation
- PulseoximetryDocument2 pagesPulseoximetryRakshith NagarajaiahPas encore d'évaluation
- Urine Case 2010-2Document9 pagesUrine Case 2010-2hendra_darmawan_4Pas encore d'évaluation
- Daftar PustakaDocument2 pagesDaftar PustakaameliaaarrPas encore d'évaluation
- Career 1Document2 pagesCareer 1api-387334532Pas encore d'évaluation
- Accupressure Points Chart PDFDocument20 pagesAccupressure Points Chart PDFshule1100% (2)
- Short Essay On ObesityDocument6 pagesShort Essay On ObesityLisa Wong100% (1)
- Q3-Las-Health10-Module 3-Weeks 6-8Document6 pagesQ3-Las-Health10-Module 3-Weeks 6-8MA TEODORA CABEZADAPas encore d'évaluation