Vous aimerez peut-être aussi
- Westlife - My Love Song LyricsDocument2 pagesWestlife - My Love Song LyricsBuddy ArifPas encore d'évaluation
- Health Panel Seeks Sweeping Changes in Fertility TherapyDocument4 pagesHealth Panel Seeks Sweeping Changes in Fertility Therapyrahmawati aliwarmanPas encore d'évaluation
- When You Tell Me That Ou Love MeDocument2 pagesWhen You Tell Me That Ou Love Merahmawati aliwarmanPas encore d'évaluation
- Without You (Reference Vocal) : Posting Lirik Ini Di Blog AndaDocument1 pageWithout You (Reference Vocal) : Posting Lirik Ini Di Blog Andarahmawati aliwarmanPas encore d'évaluation
- F24 - Epilepsy After StrokeDocument6 pagesF24 - Epilepsy After StrokeplocnicuPas encore d'évaluation
- Facts About Chikungunya17806 PDFDocument6 pagesFacts About Chikungunya17806 PDFNitin NaharPas encore d'évaluation
- Bhattacharyya BPPV CPGDocument35 pagesBhattacharyya BPPV CPGrahmawati aliwarmanPas encore d'évaluation
- What Is RH IncompatibilityDocument30 pagesWhat Is RH Incompatibilityrahmawati aliwarmanPas encore d'évaluation
- CREZIERDocument1 pageCREZIERrahmawati aliwarmanPas encore d'évaluation
- 10 5923 J Ajdv 20150403 01Document3 pages10 5923 J Ajdv 20150403 01rahmawati aliwarmanPas encore d'évaluation
- All by MyselfDocument2 pagesAll by Myselfrahmawati aliwarmanPas encore d'évaluation
- Desviat 2006 CcaDocument4 pagesDesviat 2006 Ccarahmawati aliwarmanPas encore d'évaluation
- MelasmaDocument5 pagesMelasmarahmawati aliwarmanPas encore d'évaluation
- JCN 11 E34Document8 pagesJCN 11 E34kakarafniePas encore d'évaluation
- Vertigo diagnosis and management in primary careDocument3 pagesVertigo diagnosis and management in primary careAacg MeryendPas encore d'évaluation
- 38 Acne PDFDocument7 pages38 Acne PDFRamadhan Harya Puja KusumaPas encore d'évaluation
- All by MyselfDocument2 pagesAll by Myselfrahmawati aliwarmanPas encore d'évaluation
- Histamine Antagonists For Treatment of Peripheral Vertigo: A Meta-AnalysisDocument5 pagesHistamine Antagonists For Treatment of Peripheral Vertigo: A Meta-Analysisrahmawati aliwarmanPas encore d'évaluation
- JCN 11 262Document6 pagesJCN 11 262rahmawati aliwarmanPas encore d'évaluation
- True Vertigo Patients in Emergency Department An Epidemiologic StudyDocument4 pagesTrue Vertigo Patients in Emergency Department An Epidemiologic Studyrahmawati aliwarmanPas encore d'évaluation
- The Analysis of The Mycobacterium Leprae Resistance Against Ofloxacin After The Rifampicin Ofloxacin Minocycline (ROM) TherapyDocument5 pagesThe Analysis of The Mycobacterium Leprae Resistance Against Ofloxacin After The Rifampicin Ofloxacin Minocycline (ROM) Therapyrahmawati aliwarmanPas encore d'évaluation
- 1 SS Skin Cancer - Chapter 1Document12 pages1 SS Skin Cancer - Chapter 1Muhammad IqbalPas encore d'évaluation
- Should We Use Ceftriaxone To Treat Staphylococcal.2Document2 pagesShould We Use Ceftriaxone To Treat Staphylococcal.2rahmawati aliwarmanPas encore d'évaluation
- Sel KeratinositDocument6 pagesSel KeratinositChristover Firstnando Saragih SimarmataPas encore d'évaluation
- Pi Is 0002934300004125Document8 pagesPi Is 0002934300004125rahmawati aliwarmanPas encore d'évaluation
- Bawang Ke SaDocument14 pagesBawang Ke SaDyah Anugrah KiranaPas encore d'évaluation
- Human SkinDocument15 pagesHuman Skinrahmawati aliwarmanPas encore d'évaluation
- J. Nutr.-1992-Yamamoto-871-7Document7 pagesJ. Nutr.-1992-Yamamoto-871-7rahmawati aliwarmanPas encore d'évaluation
- Correspondence: Methicillin-Resistant Staphylococcus Aureus Clinical Strain With Reduced Vancomycin SusceptibilityDocument12 pagesCorrespondence: Methicillin-Resistant Staphylococcus Aureus Clinical Strain With Reduced Vancomycin Susceptibilityrahmawati aliwarmanPas encore d'évaluation
- 5 and Type 8 Capsular Polysaccharides by Type Regulation Of: Staphylococcus AureusDocument6 pages5 and Type 8 Capsular Polysaccharides by Type Regulation Of: Staphylococcus Aureusrahmawati aliwarmanPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Level 2. How Do Cigarettes Affect The Body - Krishna SudhirDocument3 pagesLevel 2. How Do Cigarettes Affect The Body - Krishna SudhirELIBERTO FIGUEROA OMEPas encore d'évaluation
- ANRAP Announcement PDFDocument1 pageANRAP Announcement PDFBuddhi Bal ChidiPas encore d'évaluation
- PsychopathologyDocument298 pagesPsychopathologyAlguémPas encore d'évaluation
- 3, Prof. Brendon Kearney - Health Technology AssessmentDocument19 pages3, Prof. Brendon Kearney - Health Technology Assessmentave mariaPas encore d'évaluation
- Step Test Aerobic Fitness MeasureDocument1 pageStep Test Aerobic Fitness MeasureJerico Villa MaglasangPas encore d'évaluation
- All Questions To Be Answered. Each Question To Be Answered in A Separate Book (Or Books If More Than One Is Required For The One Answer)Document3 pagesAll Questions To Be Answered. Each Question To Be Answered in A Separate Book (Or Books If More Than One Is Required For The One Answer)matentenPas encore d'évaluation
- BFR PicoDocument1 pageBFR PicoErLz Catubig AlmendralPas encore d'évaluation
- Strategies For Dengue Control ProgramDocument22 pagesStrategies For Dengue Control ProgramNaseem QaziPas encore d'évaluation
- TtexDocument26 pagesTtexGlen DizonPas encore d'évaluation
- Suvendu Hota Cowin CertificateDocument1 pageSuvendu Hota Cowin CertificateHemalika SharmaPas encore d'évaluation
- OMSC First Aid & Water Safety Activities DocumentDocument4 pagesOMSC First Aid & Water Safety Activities DocumentPablito GuachePas encore d'évaluation
- Fess StorzDocument2 pagesFess StorzdarmawanPas encore d'évaluation
- ComprehensiveUnifiedPolicy TBDocument159 pagesComprehensiveUnifiedPolicy TBallan14_reyesPas encore d'évaluation
- Cognitive Behavioral Therapy For Managing PainDocument3 pagesCognitive Behavioral Therapy For Managing PainJustus K GatheruPas encore d'évaluation
- NCDPD Script Implementation Recommendations V 127Document102 pagesNCDPD Script Implementation Recommendations V 127john mullerPas encore d'évaluation
- Employee EngagementDocument20 pagesEmployee EngagementVaishnavi KhandelwalPas encore d'évaluation
- D-dimer and platelet aggregation predict thrombotic risk in PADDocument8 pagesD-dimer and platelet aggregation predict thrombotic risk in PADlidawatiPas encore d'évaluation
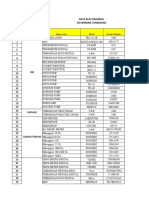
- Data Alat Kalibrasi Rs TNGDocument10 pagesData Alat Kalibrasi Rs TNGHelena LowaPas encore d'évaluation
- Acute Migraine Treatment.6Document16 pagesAcute Migraine Treatment.6BryanPas encore d'évaluation
- Comminuted Patella FracturesDocument8 pagesComminuted Patella FracturesKirana lupitaPas encore d'évaluation
- NCP For Bipolar Risk For Injury Related To Extreme Hyperactivity As Evidenced by Excessive and Constant Motor ActivityDocument3 pagesNCP For Bipolar Risk For Injury Related To Extreme Hyperactivity As Evidenced by Excessive and Constant Motor Activitydana75% (4)
- Laser Retinopexy PDFDocument4 pagesLaser Retinopexy PDFveerroxxPas encore d'évaluation
- Drugs Affecting Respiratory SystemDocument62 pagesDrugs Affecting Respiratory Systemyunita ekawatiPas encore d'évaluation
- Fever: Clinical DescriptionDocument6 pagesFever: Clinical DescriptionNama ManaPas encore d'évaluation
- PericarditisDocument19 pagesPericarditisxmitchxPas encore d'évaluation
- Laporan Pelayanan Rawat Jalan Pertama (RJPT) BULAN TAHUN .. Nama Faskes: Puskesmas Amahai Alamat: SoahukuDocument35 pagesLaporan Pelayanan Rawat Jalan Pertama (RJPT) BULAN TAHUN .. Nama Faskes: Puskesmas Amahai Alamat: SoahukuEnggelberth WattimenaPas encore d'évaluation
- DIBDDocument11 pagesDIBDKabirPas encore d'évaluation
- 21Document177 pages21Carlos HernándezPas encore d'évaluation
- Atresia BilieerDocument9 pagesAtresia BilieerSolo UpdatePas encore d'évaluation