Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Professional Development PlanDocument2 pagesProfessional Development Planapi-245887979100% (1)
- Assessment Nursing Diagnosis Outcome Identification Planning Intervention Rationale Evaluation Subjective Data: Short Term: IndependentDocument2 pagesAssessment Nursing Diagnosis Outcome Identification Planning Intervention Rationale Evaluation Subjective Data: Short Term: IndependentDimple Castañeto Callo100% (1)
- Southwestern University - PRC FormatDocument15 pagesSouthwestern University - PRC FormatemytheresePas encore d'évaluation
- Laboratory Activity - HIS Lab - IDTOMISDocument2 pagesLaboratory Activity - HIS Lab - IDTOMISFrance Cedrick RamosPas encore d'évaluation
- Nabh Application Diagnostic Laboratories Imaging Centres PDFDocument35 pagesNabh Application Diagnostic Laboratories Imaging Centres PDFPrateek ChaharPas encore d'évaluation
- Jurnal MassageDocument8 pagesJurnal MassageDyah PridamiPas encore d'évaluation
- Patient Safety Is Our Top PriorityDocument14 pagesPatient Safety Is Our Top PriorityAlexandre SouzaPas encore d'évaluation
- Form of Application For Claiming Reimbursement of Medical Expenses of Government Servants and Their FamiliesDocument5 pagesForm of Application For Claiming Reimbursement of Medical Expenses of Government Servants and Their FamiliesAmit GautamPas encore d'évaluation
- Courier: A Thousand WordsDocument20 pagesCourier: A Thousand WordsAnonymous 9eadjPSJNgPas encore d'évaluation
- Ampullary Carcinoma: Treatment and PrognosisDocument24 pagesAmpullary Carcinoma: Treatment and PrognosisHugo Alves100% (1)
- Section 12Document7 pagesSection 12Saravanan ThangarajanPas encore d'évaluation
- NURS449 Clinical Preceptorship PurposeDocument3 pagesNURS449 Clinical Preceptorship PurposeAmeng GosimPas encore d'évaluation
- Prescription WritingDocument28 pagesPrescription WritingEshana AryaPas encore d'évaluation
- International Journal of Surgery Open: Amir Forouzanfar, Jonathan Smith, Keith S. ChappleDocument3 pagesInternational Journal of Surgery Open: Amir Forouzanfar, Jonathan Smith, Keith S. ChappleSiti Fildzah NadhilahPas encore d'évaluation
- FIGO Cancer Report 2018Document2 pagesFIGO Cancer Report 2018Anonymous 2XsadJlrPas encore d'évaluation
- Vaccination Workforce Briefing - 210113Document12 pagesVaccination Workforce Briefing - 210113Scott BilleckPas encore d'évaluation
- Official Medical Information and Release FormDocument2 pagesOfficial Medical Information and Release FormtheNOLAtreePas encore d'évaluation
- National Preparedness and Response Plan For COVID 19, BangladeshDocument46 pagesNational Preparedness and Response Plan For COVID 19, BangladeshAmena Jahan UrmyPas encore d'évaluation
- Biostat ManipalDocument4 pagesBiostat ManipalVijay KumarPas encore d'évaluation
- IBO - Information For CandidatesDocument10 pagesIBO - Information For Candidatesdrzana78Pas encore d'évaluation
- Ethical Issues and The ElderlyDocument15 pagesEthical Issues and The Elderlythanuja mathewPas encore d'évaluation
- Probiotic Evidence ReportDocument645 pagesProbiotic Evidence ReportThiago PessoaPas encore d'évaluation
- TL3 8 Garbim2021Document33 pagesTL3 8 Garbim2021bomonnhacongdongPas encore d'évaluation
- Management of Dental Emergencies in Children and Adolescents - 2019 - Neuhaus PDFDocument296 pagesManagement of Dental Emergencies in Children and Adolescents - 2019 - Neuhaus PDFFran GidiPas encore d'évaluation
- Assessment of Factors Affecting Child Art Adherence Among Children Attending Jimma University Specialized Hospital, Art ClinicDocument31 pagesAssessment of Factors Affecting Child Art Adherence Among Children Attending Jimma University Specialized Hospital, Art Clinickelid IbrahimPas encore d'évaluation
- 1mg BillDocument1 page1mg BillkgagansinghPas encore d'évaluation
- Policies and ProceduresDocument24 pagesPolicies and ProceduresAbdulazizPas encore d'évaluation
- Nursing CompetenciesDocument22 pagesNursing CompetenciesBishwajitMazumderPas encore d'évaluation
- GOVERNMENT SAMPLES - Selection Criteria 3-5 PagesDocument24 pagesGOVERNMENT SAMPLES - Selection Criteria 3-5 PagesRakesh Nisha Lakhanpal0% (1)
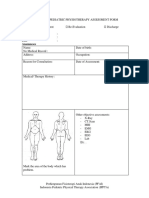
- Form PEMERIKSANAAN UMUM FT ANAK 300419Document4 pagesForm PEMERIKSANAAN UMUM FT ANAK 300419vanoPas encore d'évaluation