Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Pustjens2020 Article GuidelinesForTheManagementOfMyDocument15 pagesPustjens2020 Article GuidelinesForTheManagementOfMyganangahimsaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Differential Diagnosis of Cardiogenic Syncope and Seizure DisordersDocument6 pagesDifferential Diagnosis of Cardiogenic Syncope and Seizure DisordersganangahimsaPas encore d'évaluation
- Abstracts: Case Reports: Indonesian Journal of CardiologyDocument63 pagesAbstracts: Case Reports: Indonesian Journal of CardiologyganangahimsaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- References: Left Ventricular Thrombus Sans Overt Cardiac PathologyDocument3 pagesReferences: Left Ventricular Thrombus Sans Overt Cardiac PathologyganangahimsaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Combining Oral Anticoagulants With Atrial FibriaaionDocument11 pagesCombining Oral Anticoagulants With Atrial FibriaaionganangahimsaPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Mostafa Et - at - Factors Affecting RestenosisDocument8 pagesMostafa Et - at - Factors Affecting RestenosisNo ObPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Regulatory Effector T Cell Ratio in Reduce CADDocument7 pagesRegulatory Effector T Cell Ratio in Reduce CADganangahimsaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Amer Fam Phys GallstonesDocument7 pagesAmer Fam Phys GallstonesganangahimsaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Endokrin Journal ReadingDocument28 pagesEndokrin Journal ReadingganangahimsaPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Surviving Sepsis Campaign International.15Document67 pagesSurviving Sepsis Campaign International.15Tanawat SingboonPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Triatmo Budiyuwono SPJP (K), FIHA, FAPSICDocument40 pagesTriatmo Budiyuwono SPJP (K), FIHA, FAPSICganangahimsaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- APM211 13 RuptureDocument3 pagesAPM211 13 RuptureganangahimsaPas encore d'évaluation
- Comparative Safety of Sulfonylurea and Metformin Monotherapy On The Risk of Heart Failure: A Cohort StudyDocument29 pagesComparative Safety of Sulfonylurea and Metformin Monotherapy On The Risk of Heart Failure: A Cohort StudyganangahimsaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Anti Inflamatory and Immune Modulatory Therapy For Preenting Atherosclerotic CVDocument8 pagesAnti Inflamatory and Immune Modulatory Therapy For Preenting Atherosclerotic CVganangahimsaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Hansson Et Al The Immune Response in AtherosclerosisDocument12 pagesHansson Et Al The Immune Response in AtherosclerosisStavros GiaglisPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Regulatory Effector T Cell Ratio in Reduce CADDocument7 pagesRegulatory Effector T Cell Ratio in Reduce CADganangahimsaPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Protective Imunity in AtherosleloticDocument73 pagesProtective Imunity in AtherosleloticganangahimsaPas encore d'évaluation
- Immunity Atherosclerosis and CVDDocument13 pagesImmunity Atherosclerosis and CVDganangahimsaPas encore d'évaluation
- Regulatory T Cell I AtheroschlerisisDocument13 pagesRegulatory T Cell I AtheroschlerisisganangahimsaPas encore d'évaluation
- Dendritic Cell in AtheroscleroticDocument9 pagesDendritic Cell in AtheroscleroticganangahimsaPas encore d'évaluation
- Flow Pattern at Stented Coronary BifurcationDocument11 pagesFlow Pattern at Stented Coronary BifurcationganangahimsaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Willmott Et Al-2008-BJOG An International Journal of Obstetrics & GynaecologyDocument3 pagesWillmott Et Al-2008-BJOG An International Journal of Obstetrics & GynaecologyganangahimsaPas encore d'évaluation
- Uterine Rupture in Second-Trimester Misoprostol-Induced Abortion After Cesarean DeliveryDocument7 pagesUterine Rupture in Second-Trimester Misoprostol-Induced Abortion After Cesarean DeliveryganangahimsaPas encore d'évaluation
- Arterioscler Thromb Vasc Biol 2011 Nakajima 1963 72Document20 pagesArterioscler Thromb Vasc Biol 2011 Nakajima 1963 72ganangahimsaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- 2714Document3 pages2714ganangahimsaPas encore d'évaluation
- Reproductive Toxicology Volume 20 Issue 4 2005 (Doi 10.1016/j.reprotox.2005.04.014) Joo Oh Kim Jung Yeol Han June Seek Choi Hyun Kyong Ahn Jae H - Oral Misoprostol and Uterine Rupture in The FiDocument3 pagesReproductive Toxicology Volume 20 Issue 4 2005 (Doi 10.1016/j.reprotox.2005.04.014) Joo Oh Kim Jung Yeol Han June Seek Choi Hyun Kyong Ahn Jae H - Oral Misoprostol and Uterine Rupture in The FiganangahimsaPas encore d'évaluation
- 2714Document3 pages2714ganangahimsaPas encore d'évaluation
- A7 PDFDocument49 pagesA7 PDFganangahimsaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Konsep Diri Odha Wilayah PKM SrandakanDocument1 pageKonsep Diri Odha Wilayah PKM SrandakanganangahimsaPas encore d'évaluation
- A7 PDFDocument49 pagesA7 PDFganangahimsaPas encore d'évaluation
- Salma Math 1Document7 pagesSalma Math 1Tuti AlawiahPas encore d'évaluation
- NCMB 312 - : Bachelor of Science in Nursing Communicable Disease NursingDocument17 pagesNCMB 312 - : Bachelor of Science in Nursing Communicable Disease NursingDona Mae TaberaPas encore d'évaluation
- Communicable Disease NursingDocument28 pagesCommunicable Disease NursingCyrin Once100% (2)
- Pedia-Reviewer CompleteDocument36 pagesPedia-Reviewer CompletePotato BroPas encore d'évaluation
- (10920684 - Neurosurgical Focus) Intracranial Infections - Lessons Learned From 52 Surgically Treated CasesDocument8 pages(10920684 - Neurosurgical Focus) Intracranial Infections - Lessons Learned From 52 Surgically Treated CasesIsmail MuhammadPas encore d'évaluation
- Microbial Diseases of The Different Organ System and Epidem.Document36 pagesMicrobial Diseases of The Different Organ System and Epidem.Ysabelle GutierrezPas encore d'évaluation
- Early-Onset Sepsis :clinical and Laboratory ChallengeDocument34 pagesEarly-Onset Sepsis :clinical and Laboratory ChallengelordofthewebPas encore d'évaluation
- WHO Fact Sheet Emerging and Re Emerging Infectious Disease Agustus 1998Document7 pagesWHO Fact Sheet Emerging and Re Emerging Infectious Disease Agustus 1998Amanda PratiwiPas encore d'évaluation
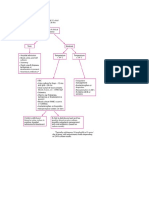
- Concept Map 1 - PedsDocument4 pagesConcept Map 1 - Pedsv0912040525Pas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Clinical MicrobiologyDocument91 pagesClinical MicrobiologyDr. Jayesh Patidar67% (3)
- Chapter 59: Nursing Management: Acute Intracranial Problems Lewis Et Al.: Medical-Surgical Nursing in Canada, 3rd EditionDocument14 pagesChapter 59: Nursing Management: Acute Intracranial Problems Lewis Et Al.: Medical-Surgical Nursing in Canada, 3rd EditionlmaoheartsPas encore d'évaluation
- Dermatology Videos by DR RihamDocument31 pagesDermatology Videos by DR Rihamengr_shazzPas encore d'évaluation
- MedFit Form (JAL)Document4 pagesMedFit Form (JAL)FrancescoBarberoPas encore d'évaluation
- Bacterial Meningitis in ChildrenDocument10 pagesBacterial Meningitis in ChildrenAnny AryanyPas encore d'évaluation
- Acute Bacterial Meningitis in ChildrenDocument48 pagesAcute Bacterial Meningitis in ChildrenRadhika BatraPas encore d'évaluation
- UHSDocument13 pagesUHSLatif RanaPas encore d'évaluation
- Lesson Plan Lumbar PunctureDocument19 pagesLesson Plan Lumbar PunctureLoma Waghmare (Jadhav)Pas encore d'évaluation
- A Case Study of "Meningitis": Mary Chiles College Gastambide St. Sampaloc ManilaDocument16 pagesA Case Study of "Meningitis": Mary Chiles College Gastambide St. Sampaloc ManilaJessa BorrePas encore d'évaluation
- Viral Meningitis: Current Issues in Diagnosis and TreatmentDocument9 pagesViral Meningitis: Current Issues in Diagnosis and Treatmentrisna sariPas encore d'évaluation
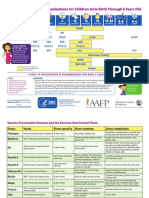
- Parent Ver SCH 0 6yrs AafpDocument2 pagesParent Ver SCH 0 6yrs AafpcicitPas encore d'évaluation
- Algoritma Fever, DLLDocument4 pagesAlgoritma Fever, DLLVanDoctor JerseyPas encore d'évaluation
- Case Analysis Viral Meningitis 1Document75 pagesCase Analysis Viral Meningitis 1Jenylyn AlingPas encore d'évaluation
- Med SurgDocument5 pagesMed SurgSherilPas encore d'évaluation
- Nursing Care Plan Pedia TB MeningitisDocument2 pagesNursing Care Plan Pedia TB Meningitisderic100% (10)
- Pediatric SeizuresDocument103 pagesPediatric SeizuresDanielle Ban100% (1)
- Neonate: TPR of Newborns BW 1500gDocument9 pagesNeonate: TPR of Newborns BW 1500gAnne Lorraine BringasPas encore d'évaluation
- Infectious Diseases Student Handbook 2019Document17 pagesInfectious Diseases Student Handbook 2019Warren SeowPas encore d'évaluation
- Ilovepdf MergedDocument45 pagesIlovepdf Mergedacte minophenPas encore d'évaluation
- Lumbar Puncture GuidelinesDocument6 pagesLumbar Puncture GuidelinesYwagar YwagarPas encore d'évaluation
- Bacterial Men CPGDocument42 pagesBacterial Men CPGKarl Jimenez SeparaPas encore d'évaluation
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)