Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Mapeh 4th Quarter ExamDocument3 pagesMapeh 4th Quarter ExamJohn DiestroPas encore d'évaluation
- Cytology I - Techniques and Application: Peter NG Cyto Lab Ic, MT, PYNEHDocument201 pagesCytology I - Techniques and Application: Peter NG Cyto Lab Ic, MT, PYNEHbusiness onlyyouPas encore d'évaluation
- 3 Nursing Diagnosis and Nursing Interventions ForDocument2 pages3 Nursing Diagnosis and Nursing Interventions ForSharmaine Grace Florig67% (3)
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument8 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiPas encore d'évaluation
- Cyclotron Booklet Black Final PrintDocument10 pagesCyclotron Booklet Black Final PrintNawaf BamasoudPas encore d'évaluation
- Gastric AdenocarcinomaDocument1 pageGastric AdenocarcinomaIjenaePas encore d'évaluation
- (Attachment 3) Data Sheet - ELRA ElectrodeDocument2 pages(Attachment 3) Data Sheet - ELRA Electroderaul apolinarPas encore d'évaluation
- Leydig Cells TumoursDocument3 pagesLeydig Cells TumoursVladislav GramaPas encore d'évaluation
- Ovarian Cancer ThesisDocument8 pagesOvarian Cancer ThesisDon Dooley100% (1)
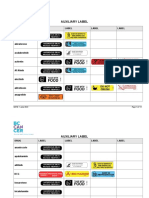
- Auxiliary Label LISTDocument14 pagesAuxiliary Label LISTAbdur RachmanPas encore d'évaluation
- Can Squeezing Your Breadt Realease Stress - Google Search PDFDocument1 pageCan Squeezing Your Breadt Realease Stress - Google Search PDFJennifer LimaPas encore d'évaluation
- A04P600 - DV610K - en - 2016 SdsDocument7 pagesA04P600 - DV610K - en - 2016 SdsJohan WolfensteinPas encore d'évaluation
- LUNG CaDocument59 pagesLUNG CaokaciaPas encore d'évaluation
- Pelvic Lymphadenectomy Step-By-Step Surgical EducaDocument5 pagesPelvic Lymphadenectomy Step-By-Step Surgical EducaVlad GrigorePas encore d'évaluation
- The Bizarre Case of Warthins Tumor in Submandibular Gland-Case ReportDocument9 pagesThe Bizarre Case of Warthins Tumor in Submandibular Gland-Case ReportInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Clinical Spectrum and Dermoscopic Features of Seborrheic KeratosisDocument1 pageClinical Spectrum and Dermoscopic Features of Seborrheic KeratosisRicky SetiawanPas encore d'évaluation
- Mad-000550q - 171120 - 835 - Mad-000550 FT en 2020-09-21Document2 pagesMad-000550q - 171120 - 835 - Mad-000550 FT en 2020-09-21Anca NeaguPas encore d'évaluation
- Wilms Tumor: Imaging of Pediatric Renal MassesDocument35 pagesWilms Tumor: Imaging of Pediatric Renal MassesEnny AndrianiPas encore d'évaluation
- Colorectal Cancer (CRC)Document51 pagesColorectal Cancer (CRC)Rexhail RamadaniPas encore d'évaluation
- Protig 205Document32 pagesProtig 205Dale BergerPas encore d'évaluation
- Jurnal Akper Buntet Jurnal Ilmiah Akper Buntet Pesantren Cirebon ISSN: 2579-3837 Vol. 2 No. 1 2018Document16 pagesJurnal Akper Buntet Jurnal Ilmiah Akper Buntet Pesantren Cirebon ISSN: 2579-3837 Vol. 2 No. 1 2018Lamria PakpahanPas encore d'évaluation
- Intl Journal of Cancer - 2004 - Capasso - Antiquity of CancerDocument13 pagesIntl Journal of Cancer - 2004 - Capasso - Antiquity of CancerPilar AufrastoPas encore d'évaluation
- Squamous Cell CarcinomaDocument7 pagesSquamous Cell CarcinomaMihnea NaşcaPas encore d'évaluation
- A Case - Control Study of Smoking and Bladder Cancer RiskDocument9 pagesA Case - Control Study of Smoking and Bladder Cancer RiskHuy Nguyễn NhậtPas encore d'évaluation
- Critical SkillsDocument5 pagesCritical SkillsJosiah MwashitaPas encore d'évaluation
- Anatomy and Physiology of Colon of Case StudyDocument4 pagesAnatomy and Physiology of Colon of Case StudySimran JosanPas encore d'évaluation
- Lecture-4 The Molecular Basis of Cancer Part-3Document19 pagesLecture-4 The Molecular Basis of Cancer Part-3samyPas encore d'évaluation
- Gastrointestinal Stromal TumoursDocument22 pagesGastrointestinal Stromal TumoursThomas KlebPas encore d'évaluation
- Cancer Lead Generation ScriptDocument2 pagesCancer Lead Generation ScriptJamal AliPas encore d'évaluation
- Manual Vacuum AspirationDocument3 pagesManual Vacuum AspirationDredd Alejo SumbadPas encore d'évaluation