Vous aimerez peut-être aussi
- The LarynxDocument60 pagesThe LarynxAbeer RadiPas encore d'évaluation
- Guide to Laryngoscopy Exam of the Voice BoxDocument3 pagesGuide to Laryngoscopy Exam of the Voice BoxShazPas encore d'évaluation
- Anatomy RfeviewDocument2 pagesAnatomy Rfeviewgreen matePas encore d'évaluation
- Hernia: DR - Surender Singh DhankharDocument36 pagesHernia: DR - Surender Singh DhankharBharat BhushanPas encore d'évaluation
- GS2 HerniaDocument13 pagesGS2 HerniaMAH pedPas encore d'évaluation
- Krishna Reddy Anatomy of PharynxDocument20 pagesKrishna Reddy Anatomy of PharynxSiva ramaPas encore d'évaluation
- Tracheostomy Operating TechniqueDocument34 pagesTracheostomy Operating TechniqueIsa BasukiPas encore d'évaluation
- 4 LaryngologyDocument116 pages4 LaryngologyWai Kwong ChiuPas encore d'évaluation
- Abdominal Wall Learning ObjectivesDocument7 pagesAbdominal Wall Learning ObjectivesMadison KommorPas encore d'évaluation
- LBM 5 THT SGD 15Document42 pagesLBM 5 THT SGD 15Akhmad Ulil AlbabPas encore d'évaluation
- Phraynx FinalDocument54 pagesPhraynx FinalAbdullah NayyarPas encore d'évaluation
- Presentasi Jurnal LaryngoceleDocument13 pagesPresentasi Jurnal LaryngoceleTiara Rachmaputeri AriantoPas encore d'évaluation
- Head Neck-Pharynx Larynx Thyroid GlandDocument8 pagesHead Neck-Pharynx Larynx Thyroid GlandMe MyselfPas encore d'évaluation
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- LARYNX ANATOMYDocument83 pagesLARYNX ANATOMYGeraldine Marie SalvoPas encore d'évaluation
- Head and NeckDocument21 pagesHead and NeckUday PrabhuPas encore d'évaluation
- Airway BSC AnesthesiaDocument72 pagesAirway BSC AnesthesiaTerefe AlemayehuPas encore d'évaluation
- Larynx Wrote by DR Nassem TalaatDocument38 pagesLarynx Wrote by DR Nassem TalaatAbouzr Mohammed ElsaidPas encore d'évaluation
- Practice Quiz - Carotid Sheath, Pharynx, & LarynxDocument4 pagesPractice Quiz - Carotid Sheath, Pharynx, & LarynxWongani ZuluPas encore d'évaluation
- Airway TraumaDocument73 pagesAirway TraumaSarah BirechPas encore d'évaluation
- LaryngoceleDocument7 pagesLaryngoceleM Grecu CeptureanuPas encore d'évaluation
- Multiple Trauma Case ManagementDocument24 pagesMultiple Trauma Case Managementsylvia haryantoPas encore d'évaluation
- Total LaryngectomyDocument15 pagesTotal LaryngectomyDenny Rizaldi AriantoPas encore d'évaluation
- Laryngomalacia - PPTX Dr. FeriDocument114 pagesLaryngomalacia - PPTX Dr. FeriAldy BimaPas encore d'évaluation
- Everything You Need to Know About HerniasDocument47 pagesEverything You Need to Know About HerniasmalathiPas encore d'évaluation
- HerniaDocument46 pagesHerniaZubairkhan SuraniPas encore d'évaluation
- Esophagus Guide: Embryology, Anatomy, Exams & MoreDocument14 pagesEsophagus Guide: Embryology, Anatomy, Exams & MoreDave AbrahamPas encore d'évaluation
- Scrotal MassesDocument19 pagesScrotal MassesJohnPas encore d'évaluation
- Airway ObstructionDocument32 pagesAirway ObstructionAmirrah LaurentePas encore d'évaluation
- Practice Quiz - Anterior Triangle of The NeckDocument7 pagesPractice Quiz - Anterior Triangle of The NeckWongani ZuluPas encore d'évaluation
- Ent Throat 1Document58 pagesEnt Throat 1ميمونه عبدالرحيم مصطفىPas encore d'évaluation
- Anatomy Physio AnesthesiaDocument6 pagesAnatomy Physio AnesthesiaMarites L. DomingoPas encore d'évaluation
- L13 - Diseases of LarynxI&IIDocument90 pagesL13 - Diseases of LarynxI&IINouf Al-orainiPas encore d'évaluation
- Hernia: Done by D1 GroupDocument47 pagesHernia: Done by D1 Groupanindyadputri100% (1)
- 1092_Endotracheal-IntubationDocument25 pages1092_Endotracheal-IntubationTiban ParthibanPas encore d'évaluation
- Congenital Anomalies of Airway and Lung ParenchymaDocument71 pagesCongenital Anomalies of Airway and Lung ParenchymaGopal ChawlaPas encore d'évaluation
- Imperforate Anus and Cloacal MalformationsDocument110 pagesImperforate Anus and Cloacal MalformationsAhmad Abu KushPas encore d'évaluation
- Respiratory AssessmentDocument54 pagesRespiratory Assessmentraima ayazPas encore d'évaluation
- Thyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandThyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- ENT - Essays - Sun 2016Document6 pagesENT - Essays - Sun 2016rabeca johnsonPas encore d'évaluation
- HerniaDocument26 pagesHerniaSudhanshu ShekharPas encore d'évaluation
- Pharyanx IDocument28 pagesPharyanx Ij8bhfmc6s9Pas encore d'évaluation
- Manejo Via AeraDocument6 pagesManejo Via AeraCarolin SantosPas encore d'évaluation
- Head Neck Face-13 (Larynx and Deep Neck Structures)Document47 pagesHead Neck Face-13 (Larynx and Deep Neck Structures)spitzmark2030Pas encore d'évaluation
- Total Thyroidectomy - EdittedDocument55 pagesTotal Thyroidectomy - EdittedPrisicilla Doydora Pat67% (3)
- E T IntubationDocument15 pagesE T Intubationjtalan9Pas encore d'évaluation
- Open Inguinal Hernia RepairDocument6 pagesOpen Inguinal Hernia RepairKris TejereroPas encore d'évaluation
- Zenker's DiverticulumDocument3 pagesZenker's Diverticulumnevelle4667Pas encore d'évaluation
- Anatomy and Physiology of LarynxDocument37 pagesAnatomy and Physiology of Larynxsuci100% (1)
- Anaesthesia SummaryDocument36 pagesAnaesthesia SummaryRazan QassemPas encore d'évaluation
- Anatomy of the Head and Neck StructuresDocument76 pagesAnatomy of the Head and Neck StructuresJeff GonzalesPas encore d'évaluation
- Inguinal Hernia MinicaseDocument13 pagesInguinal Hernia MinicaseGerold Chua100% (1)
- Checklist 2Document7 pagesChecklist 2FranklinSappPas encore d'évaluation
- Consultant: Presented by DR RadheyshyamDocument60 pagesConsultant: Presented by DR RadheyshyamPriyankaPas encore d'évaluation
- ABCDE ApproachDocument7 pagesABCDE ApproachmariamPas encore d'évaluation
- Natomy of Larynx: Moderator: DR - Manas Presenter:Ravindra.DDocument89 pagesNatomy of Larynx: Moderator: DR - Manas Presenter:Ravindra.DVandana RaviPas encore d'évaluation
- A Simple Guide to the Voice Box and Its Disorders, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to the Voice Box and Its Disorders, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- The Newer Physiology in Surgical and General PracticeD'EverandThe Newer Physiology in Surgical and General PracticePas encore d'évaluation
- From Er To Ward 1, 3, Micu: ToopdàDocument2 pagesFrom Er To Ward 1, 3, Micu: ToopdàJay VeePas encore d'évaluation
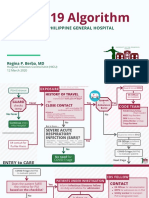
- COVID-19 Algorithm: For The Philippine General HospitalDocument10 pagesCOVID-19 Algorithm: For The Philippine General HospitalJay VeePas encore d'évaluation
- Sample Medical Guidelines: Congestive Heart FailureDocument2 pagesSample Medical Guidelines: Congestive Heart FailureJohanna ShuulukaPas encore d'évaluation
- PPE Selection and Use GuideDocument5 pagesPPE Selection and Use GuideJay Vee100% (1)
- K1MTZDocument1 pageK1MTZJay VeePas encore d'évaluation
- Manual-R B-Medical ClearanceDocument2 pagesManual-R B-Medical ClearanceJay VeePas encore d'évaluation
- Gym Work OutDocument19 pagesGym Work OutJay Vee100% (1)
- Emergency DashboardDocument1 pageEmergency DashboardJay VeePas encore d'évaluation
- Biological Safety Cabinet Operation and Maintenance ProceduresDocument4 pagesBiological Safety Cabinet Operation and Maintenance ProceduresJay VeePas encore d'évaluation
- RP Manual TemplateDocument9 pagesRP Manual TemplateJay VeePas encore d'évaluation
- Department of Emergency Medicine: Philippine General Hospital University of The Philippines Manila Taft Avenue, ManilaDocument1 pageDepartment of Emergency Medicine: Philippine General Hospital University of The Philippines Manila Taft Avenue, ManilaJay VeePas encore d'évaluation
- Annex 2: Laboratory Assessment Tool / Facility QuestionnaireDocument57 pagesAnnex 2: Laboratory Assessment Tool / Facility QuestionnaireJay VeePas encore d'évaluation
- Workout Set A:: Barbell Front Squat (If You Don'T Have Access, Use DBS)Document1 pageWorkout Set A:: Barbell Front Squat (If You Don'T Have Access, Use DBS)Jay VeePas encore d'évaluation
- Final Covid Guideline PsmidDocument26 pagesFinal Covid Guideline PsmidJay VeePas encore d'évaluation
- Near NCR (National Capital Region) - Quezon CityDocument1 pageNear NCR (National Capital Region) - Quezon CityJay VeePas encore d'évaluation
- CK History Final W Pe Sample MentalDocument4 pagesCK History Final W Pe Sample MentalJay VeePas encore d'évaluation
- CK History Final W Pe Sample MentalDocument4 pagesCK History Final W Pe Sample MentalJay VeePas encore d'évaluation
- Diseases of The Joint OutlineDocument1 pageDiseases of The Joint OutlineJay VeePas encore d'évaluation
- Revised Clinical HX For NewbornDocument3 pagesRevised Clinical HX For NewbornJay VeePas encore d'évaluation
- Pediatric Clinical H&PDocument7 pagesPediatric Clinical H&PJay Vee100% (1)
- Mental HealthDocument2 pagesMental HealthJay VeePas encore d'évaluation
- Pediatric History and Physical Exam GuideDocument7 pagesPediatric History and Physical Exam GuideIndunil AnuruddhikaPas encore d'évaluation
- Anesthesia Finalsurgical AnestheisaDocument66 pagesAnesthesia Finalsurgical AnestheisaJay VeePas encore d'évaluation
- Census MayDocument8 pagesCensus MayJay VeePas encore d'évaluation
- Interpleader Actions in The Ugandan Civil ProcedureDocument6 pagesInterpleader Actions in The Ugandan Civil ProcedureLevis M AtukwatsePas encore d'évaluation
- Raman Spectroscopy: 1 Theoretical BasisDocument9 pagesRaman Spectroscopy: 1 Theoretical BasisJèManziPas encore d'évaluation
- Ais 301w Resume AssignmentDocument3 pagesAis 301w Resume Assignmentapi-532849829Pas encore d'évaluation
- SEO-optimized title for practice test documentDocument4 pagesSEO-optimized title for practice test documentThu GiangPas encore d'évaluation
- Gcse English Literature Coursework Grade BoundariesDocument8 pagesGcse English Literature Coursework Grade Boundariesafjwfealtsielb100% (1)
- Ash ContentDocument2 pagesAsh Contentvikasbnsl1Pas encore d'évaluation
- Discuss in Details With Appropriate Examples What Factors Could Lead To Sympatric and Allopatric SpeciationDocument5 pagesDiscuss in Details With Appropriate Examples What Factors Could Lead To Sympatric and Allopatric SpeciationKhairul ShahmiPas encore d'évaluation
- Levenbach Causal2017Document15 pagesLevenbach Causal2017Jenna GrantPas encore d'évaluation
- Combined RubricsDocument3 pagesCombined Rubricsapi-446053878Pas encore d'évaluation
- Debt Recovery Management of SBIDocument128 pagesDebt Recovery Management of SBIpranjalamishra100% (6)
- Kung Fu MedicinesDocument9 pagesKung Fu MedicinesDavid HewittPas encore d'évaluation
- Supplier Development at Honda, Nissan and ToyotaDocument28 pagesSupplier Development at Honda, Nissan and Toyotapresidonsi100% (1)
- St. Louis ChemicalDocument8 pagesSt. Louis ChemicalNaomi Alberg-BlijdPas encore d'évaluation
- Andy Landers - Freeze Zone OffenseDocument6 pagesAndy Landers - Freeze Zone OffenseWinston Brown100% (1)
- Software Security Engineering: A Guide for Project ManagersDocument6 pagesSoftware Security Engineering: A Guide for Project ManagersVikram AwotarPas encore d'évaluation
- Conic SectionDocument58 pagesConic SectionNailah Sakinah100% (1)
- Unit Test, Part 2: Literature With A Purpose: Total Score: - of 40 PointsDocument3 pagesUnit Test, Part 2: Literature With A Purpose: Total Score: - of 40 PointsAriana Stephanya Anguiano VelazquezPas encore d'évaluation
- 50 Cool Stories 3000 Hot Words (Master Vocabulary in 50 Days) For GRE Mba Sat Banking SSC DefDocument263 pages50 Cool Stories 3000 Hot Words (Master Vocabulary in 50 Days) For GRE Mba Sat Banking SSC DefaravindPas encore d'évaluation
- What Music Really Means To ChildrenDocument5 pagesWhat Music Really Means To ChildrenMara Sofia ValentePas encore d'évaluation
- Chapter 1. Introduction To TCPIP NetworkingDocument15 pagesChapter 1. Introduction To TCPIP NetworkingPoojitha NagarajaPas encore d'évaluation
- Hitachi Datasheet Thin Image SnapshotDocument2 pagesHitachi Datasheet Thin Image Snapshotemail7urangPas encore d'évaluation
- Mil HDBK 1390 PDFDocument31 pagesMil HDBK 1390 PDFsleepanon4362Pas encore d'évaluation
- CBCP Monitor Vol. 17 No. 9Document20 pagesCBCP Monitor Vol. 17 No. 9Areopagus Communications, Inc.Pas encore d'évaluation
- Assessment Explanation of The Problem Outcomes Interventions Rationale Evaluation Sto: STO: (Goal Met)Document3 pagesAssessment Explanation of The Problem Outcomes Interventions Rationale Evaluation Sto: STO: (Goal Met)Arian May MarcosPas encore d'évaluation
- Bruno Latour: What Is Iconoclash?Document3 pagesBruno Latour: What Is Iconoclash?Clara HabibPas encore d'évaluation
- The Research TeamDocument4 pagesThe Research Teamapi-272078177Pas encore d'évaluation
- PRINCE2 Product Map Timeline Diagram (v1.5)Document11 pagesPRINCE2 Product Map Timeline Diagram (v1.5)oblonggroupPas encore d'évaluation
- Discrete Mathematics - Logical EquivalenceDocument9 pagesDiscrete Mathematics - Logical EquivalenceEisha IslamPas encore d'évaluation
- Soal Paket 1Document10 pagesSoal Paket 1Nurul HayatiPas encore d'évaluation
- Elementary Hebrew Gram 00 GreeDocument216 pagesElementary Hebrew Gram 00 GreeRobert CampoPas encore d'évaluation