Vous aimerez peut-être aussi
- Nursing Care PlansDocument7 pagesNursing Care PlansNicholaiCabadduPas encore d'évaluation
- Nursing Physical AssessmentDocument2 pagesNursing Physical Assessmentemman_abzPas encore d'évaluation
- Waiters Rhabdomyolysis PDFDocument1 pageWaiters Rhabdomyolysis PDFmp1757Pas encore d'évaluation
- NCLFNP - Mr. Robert McClelland CaseDocument4 pagesNCLFNP - Mr. Robert McClelland CaseAiresh Lamao50% (2)
- Clinical Reasoning Questions Collaboration: ConcernedDocument3 pagesClinical Reasoning Questions Collaboration: ConcernedDaniela Claire FranciscoPas encore d'évaluation
- Shadow Health Cognition SubjectiveDocument7 pagesShadow Health Cognition Subjectiveqwivy.comPas encore d'évaluation
- Manage Pain and Promote Healing for Skin InfectionDocument3 pagesManage Pain and Promote Healing for Skin InfectionReuben LouisPas encore d'évaluation
- GRP 4 CLO 2 Concept Map PT 1 PDFDocument14 pagesGRP 4 CLO 2 Concept Map PT 1 PDFMaria Lyn Ocariza ArandiaPas encore d'évaluation
- Ampicillin Med InfoDocument1 pageAmpicillin Med InfoJan McgovernPas encore d'évaluation
- Concept Map of DepressionDocument2 pagesConcept Map of DepressionJu Lie AnnPas encore d'évaluation
- NCP Fluid Volume DeficitDocument3 pagesNCP Fluid Volume DeficitNecheal BaayPas encore d'évaluation
- AnxietyDocument3 pagesAnxietyJenny Pearl Pasal100% (1)
- FOCUS CHARTING OR F-DAR CHARTINGDocument23 pagesFOCUS CHARTING OR F-DAR CHARTINGMarianne GonzalesPas encore d'évaluation
- Gerontologic Health Promotion ActivityDocument3 pagesGerontologic Health Promotion ActivityCorinne50% (2)
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaPas encore d'évaluation
- Focus Charting Example PDFDocument1 pageFocus Charting Example PDFRegine Lorenzana Mey-AngPas encore d'évaluation
- Advanced Directives: What Are They and Why Everyone Should Have OneDocument10 pagesAdvanced Directives: What Are They and Why Everyone Should Have OneEllen BriottePas encore d'évaluation
- DBFMH - Junior Staff Nurse Endorsement SheetDocument1 pageDBFMH - Junior Staff Nurse Endorsement SheetthrdPas encore d'évaluation
- Impaired Verbal and or Written CommunicationDocument2 pagesImpaired Verbal and or Written CommunicationHanya Bint Potawan100% (1)
- Internet Tools For Advanced Nursing PracticeDocument9 pagesInternet Tools For Advanced Nursing Practicesprescott01Pas encore d'évaluation
- JOb Description For SupervisorDocument2 pagesJOb Description For SupervisorJennelyn LumbrePas encore d'évaluation
- Clinical Portrait Pertinent DataDocument9 pagesClinical Portrait Pertinent DataGermin CesaPas encore d'évaluation
- NCP 3Document3 pagesNCP 3Grae TaclobPas encore d'évaluation
- Nursing Care Plan EportfolioDocument14 pagesNursing Care Plan Eportfolioapi-279212367Pas encore d'évaluation
- Risk For Falls Aeb Loss of BalanceDocument4 pagesRisk For Falls Aeb Loss of BalanceAlexandrea MayPas encore d'évaluation
- Small Bowel Obstruction Concept MapDocument1 pageSmall Bowel Obstruction Concept MapTessa Claire JaranowskiPas encore d'évaluation
- Case IcuDocument5 pagesCase IcuTrisha SuazoPas encore d'évaluation
- Abdominal Assessment VideoDocument4 pagesAbdominal Assessment VideoAmber Nicole HubbardPas encore d'évaluation
- Health Teaching Plan: EffectsDocument2 pagesHealth Teaching Plan: EffectsRheal P EsmailPas encore d'évaluation
- Staffing formula and shift optionsDocument11 pagesStaffing formula and shift optionsjoyrena ochondraPas encore d'évaluation
- Nursing Diagnosis For SeizureDocument6 pagesNursing Diagnosis For SeizureKenneth Cole100% (1)
- 10 Rights of Drug AdministrationDocument2 pages10 Rights of Drug AdministrationMike CalipayanPas encore d'évaluation
- Premenstrual Dysphoric DisorderDocument11 pagesPremenstrual Dysphoric Disorderapi-3764215Pas encore d'évaluation
- Immersion Physical Exam Final - ChecklistDocument2 pagesImmersion Physical Exam Final - ChecklistElizalde HusbandPas encore d'évaluation
- Assignment GERIATRIC ASSESSMENTDocument6 pagesAssignment GERIATRIC ASSESSMENTNur Fatima SanaaniPas encore d'évaluation
- General Appearance: Ital SignDocument4 pagesGeneral Appearance: Ital SignLiza Estrabo100% (1)
- ASSESSMENTDocument2 pagesASSESSMENTColeen PequitPas encore d'évaluation
- Nursing Care Plan Template for Student Fideli L. AbaquitaDocument1 pageNursing Care Plan Template for Student Fideli L. AbaquitafabaquitaPas encore d'évaluation
- Legal Protection of Nursing ServiceDocument4 pagesLegal Protection of Nursing ServiceJanna Kristine Ferrer Yosores80% (5)
- ER Simulation Game Self-DebriefingDocument2 pagesER Simulation Game Self-DebriefingRyrey Abraham PacamanaPas encore d'évaluation
- Spiritual and Moral ResponsibilitiesDocument206 pagesSpiritual and Moral ResponsibilitiesJoy JarinPas encore d'évaluation
- NCPDocument18 pagesNCPStephanie Villanueva AdvinculaPas encore d'évaluation
- Case Study StemiDocument2 pagesCase Study StemiRajeswari SinnasamyPas encore d'évaluation
- 1 Acute Pain NCPDocument2 pages1 Acute Pain NCPFilipinas BelzaPas encore d'évaluation
- Encouraging water consumption improves cognition in childrenDocument4 pagesEncouraging water consumption improves cognition in childrenAnnalyn MantillaPas encore d'évaluation
- Emergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Document5 pagesEmergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Wyen CabatbatPas encore d'évaluation
- Discharge PlanDocument4 pagesDischarge Plandeo_gratias14Pas encore d'évaluation
- Rathna Drug Card LisinoprilDocument1 pageRathna Drug Card Lisinoprilerdos13Pas encore d'évaluation
- Post-op Patient Fall Leads to Medical Malpractice SuitDocument7 pagesPost-op Patient Fall Leads to Medical Malpractice SuitGena RealPas encore d'évaluation
- Impaired Tissue Integrity - CellulitisDocument3 pagesImpaired Tissue Integrity - CellulitisKelvin Kurt B. AgwilangPas encore d'évaluation
- Pill-Popping Gone Bad - The Antibiotic Self-Medication Practices of Residents of Iloilo CityDocument18 pagesPill-Popping Gone Bad - The Antibiotic Self-Medication Practices of Residents of Iloilo CityBryan LadridoPas encore d'évaluation
- NCPPPPDocument6 pagesNCPPPPIvan Liquiran AvenadoPas encore d'évaluation
- General Nursing Care Plan PDFDocument17 pagesGeneral Nursing Care Plan PDFTmanoj Praveen100% (1)
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 pagesANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonPas encore d'évaluation
- Physician EvaluationDocument6 pagesPhysician Evaluationbartoncreekal100% (2)
- Chronicle Diabetes Assessment FormDocument8 pagesChronicle Diabetes Assessment FormpriyaPas encore d'évaluation
- Endocrine Students Guide-2Document2 pagesEndocrine Students Guide-2DR. MUSICPas encore d'évaluation
- IDCAP Clinical Assessment ToolsDocument4 pagesIDCAP Clinical Assessment ToolsIDCAP2011100% (1)
- Activity Intolerance: NANDA Definition Discussion of The ProblemDocument42 pagesActivity Intolerance: NANDA Definition Discussion of The Problembeautifuljade_16Pas encore d'évaluation
- Psych NCP On Risk For SuicideDocument8 pagesPsych NCP On Risk For SuicideMeagan McdonnellPas encore d'évaluation
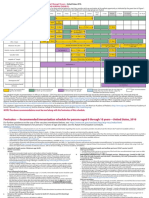
- 0 18yrs Schedule ImmunizationsDocument4 pages0 18yrs Schedule ImmunizationsIvana DobrasPas encore d'évaluation
- Atrial Septal DefekDocument19 pagesAtrial Septal DefekayounilasariPas encore d'évaluation
- Atrial Septal Defect (ASD) : What Is It?Document3 pagesAtrial Septal Defect (ASD) : What Is It?Gilbert Solomon TantonoPas encore d'évaluation
- Health AssessmentDocument25 pagesHealth AssessmentGovindaraju Subramani100% (1)
- Physical Assessment Exam Study GuideDocument35 pagesPhysical Assessment Exam Study GuideMustaf Mohamed91% (44)
- Atrial Septal Defect (ASD) : What Is It?Document3 pagesAtrial Septal Defect (ASD) : What Is It?Gilbert Solomon TantonoPas encore d'évaluation
- Improving Care For Residents With CHFDocument8 pagesImproving Care For Residents With CHFIvana Dobras100% (1)
- Priniciples of EKG InterpretationDocument26 pagesPriniciples of EKG InterpretationIvana DobrasPas encore d'évaluation
- Robb - Wolf - The Paleo Solution - The Original Human Diet PDFDocument320 pagesRobb - Wolf - The Paleo Solution - The Original Human Diet PDFGina Lenna100% (2)
- Donkey Not A HorseDocument47 pagesDonkey Not A HorseInerTiaOpheliaPas encore d'évaluation
- Casas, Jo-An Pauline A. - (LAB) Basic Concepts in NutritionDocument2 pagesCasas, Jo-An Pauline A. - (LAB) Basic Concepts in NutritionCasas, Jo-an Pauline A.Pas encore d'évaluation
- Specialist In Performance Nutrition GuideDocument24 pagesSpecialist In Performance Nutrition GuidekalikPas encore d'évaluation
- FBISE BiochemistryDocument1 pageFBISE BiochemistrySaadia AsgharPas encore d'évaluation
- BING KelompokDocument30 pagesBING KelompokMF17Pas encore d'évaluation
- Ultimate 12 Week Training System Start N PDFDocument18 pagesUltimate 12 Week Training System Start N PDFLudilan Marzano100% (1)
- Obesity Weight Loss Meal PlanDocument1 pageObesity Weight Loss Meal Planapi-607536364Pas encore d'évaluation
- Potpourri of Healing SecretsDocument11 pagesPotpourri of Healing SecretsSamee's Music100% (3)
- L11 How To Write A Good Summary AnsDocument7 pagesL11 How To Write A Good Summary Ans蘇綺晴Pas encore d'évaluation
- Whole Grains: Training For School Food Service StaffDocument20 pagesWhole Grains: Training For School Food Service StaffSafdar HussainPas encore d'évaluation
- PE NotesDocument20 pagesPE NotesAlma C WalshPas encore d'évaluation
- Vitafoods Europe 2019 New Exhibitor DirectoryDocument12 pagesVitafoods Europe 2019 New Exhibitor Directoryttquyen04Pas encore d'évaluation
- Annual Report 2008-09Document22 pagesAnnual Report 2008-09MinatiBindhaniPas encore d'évaluation
- Development of Value Added Products From Byproducts of Ethiopian Wheat Milling Industries 2157 7110 1000474Document8 pagesDevelopment of Value Added Products From Byproducts of Ethiopian Wheat Milling Industries 2157 7110 1000474Sivamani SelvarajuPas encore d'évaluation
- Q&a FinalDocument114 pagesQ&a FinalRodney MacansantosPas encore d'évaluation
- Obu Research Thesise NestleDocument46 pagesObu Research Thesise NestleHammad Ahmad100% (1)
- NCERT Class 6 Science PDFDocument167 pagesNCERT Class 6 Science PDFparvyk13Pas encore d'évaluation
- Obat MataDocument2 pagesObat MataDian EkawatiPas encore d'évaluation
- Approach To Severe Acute MalnutritionDocument49 pagesApproach To Severe Acute MalnutritionAlbertina Aipinge NandjilaPas encore d'évaluation
- Label and text comprehensionDocument1 pageLabel and text comprehensionRidaPas encore d'évaluation
- The Effect of Nutritional Supplements On OsteoarthritisDocument22 pagesThe Effect of Nutritional Supplements On OsteoarthritisRendz Pharmacist Jr.Pas encore d'évaluation
- Fitness Tracker Website Mini ProjectDocument9 pagesFitness Tracker Website Mini ProjectSrinAdh YadavPas encore d'évaluation
- SOC101 Research PaperDocument30 pagesSOC101 Research PaperJannatul Ferdousi PrïtyPas encore d'évaluation
- Revise Ros, Pe & PathoDocument8 pagesRevise Ros, Pe & PathoIrish Jane Bayle CubilloPas encore d'évaluation
- 5 Lessons from College: Stay Healthy, Build Support, Get InvolvedDocument2 pages5 Lessons from College: Stay Healthy, Build Support, Get InvolvedRaizza AcuzarPas encore d'évaluation
- W12 & W13 Lesson 15 - Common Myth and Fallacies On Exercise - ModuleDocument49 pagesW12 & W13 Lesson 15 - Common Myth and Fallacies On Exercise - ModuleShadrach AlminePas encore d'évaluation
- Policy Narratives On Food and Nutrition SecurityDocument13 pagesPolicy Narratives On Food and Nutrition SecurityInstitute of Policy StudiesPas encore d'évaluation
- Nutrition in Preschool and School AgeDocument33 pagesNutrition in Preschool and School AgeAljane Visto67% (3)