Vous aimerez peut-être aussi
- Literature of AsthmaDocument23 pagesLiterature of AsthmaAbrar Hendri PutraPas encore d'évaluation
- AsthmaDocument118 pagesAsthmaDaroo D.TPas encore d'évaluation
- Review of Related LiteratureDocument11 pagesReview of Related LiteratureLunel John RuazaPas encore d'évaluation
- Allergic RhinitisDocument27 pagesAllergic Rhinitispaningbatan.kristine.bPas encore d'évaluation
- Definisi AsmaDocument12 pagesDefinisi AsmaDayu Punik ApsariPas encore d'évaluation
- Infecciones y AsmaDocument10 pagesInfecciones y AsmadavpierPas encore d'évaluation
- ASTHMADocument17 pagesASTHMAvinda astri permatasariPas encore d'évaluation
- Allergic Rhinitis History and Presentation PDFDocument6 pagesAllergic Rhinitis History and Presentation PDFJimena LopezPas encore d'évaluation
- Childhood Asthma Diagnosis and TreatmentDocument18 pagesChildhood Asthma Diagnosis and TreatmentAlchemistalazkaPas encore d'évaluation
- Risk Factor For AllergyDocument6 pagesRisk Factor For AllergyAya AyodhiaPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument10 pagesNIH Public Access: Author ManuscriptAnnisa RahmaniPas encore d'évaluation
- Bronchial Asthma: DR Mujahid Razzaq Pediatric Medicine UCMD, UOL LahoreDocument97 pagesBronchial Asthma: DR Mujahid Razzaq Pediatric Medicine UCMD, UOL LahoreZunaira ZahraPas encore d'évaluation
- An Understanding of The Genetic Basis of Asthma: Review ArticleDocument13 pagesAn Understanding of The Genetic Basis of Asthma: Review ArticlerastiooPas encore d'évaluation
- Management of Acute Respiratory Diseases PDFDocument21 pagesManagement of Acute Respiratory Diseases PDFFernandoXavierPas encore d'évaluation
- Asthma and Food Allergy - 2019Document12 pagesAsthma and Food Allergy - 2019Cláudia SilvaPas encore d'évaluation
- Factors Linked to Rising Rates of Allergic Rhinitis and Atopic Dermatitis in ChildrenDocument11 pagesFactors Linked to Rising Rates of Allergic Rhinitis and Atopic Dermatitis in ChildrenPandu HarsarapamaPas encore d'évaluation
- Risk Factors of Allergic Rhinitis: Genetic or Environmental?Document10 pagesRisk Factors of Allergic Rhinitis: Genetic or Environmental?deirahayuPas encore d'évaluation
- Pi Is 0091674997701301Document11 pagesPi Is 0091674997701301Serque777Pas encore d'évaluation
- Investigation of The Hygiene Hypothesis: Current Issues and Future DirectionsDocument3 pagesInvestigation of The Hygiene Hypothesis: Current Issues and Future DirectionsAimee FPas encore d'évaluation
- Asthma: (Assignment 2)Document8 pagesAsthma: (Assignment 2)nuraPas encore d'évaluation
- Asthma: Whom Does It Affect?Document11 pagesAsthma: Whom Does It Affect?Ken KennyPas encore d'évaluation
- Asthma Treatment Breakthrough: Mepolizumab Relieves Severe CasesDocument8 pagesAsthma Treatment Breakthrough: Mepolizumab Relieves Severe CasesCandha NurcahyaPas encore d'évaluation
- Relationship Between Asthma and Rhinitis: Epidemiologic, Pathophysiologic, and Therapeutic AspectsDocument7 pagesRelationship Between Asthma and Rhinitis: Epidemiologic, Pathophysiologic, and Therapeutic AspectsStanley SuhermanPas encore d'évaluation
- Enviromental EffectDocument5 pagesEnviromental EffectAbdullah ZuhairPas encore d'évaluation
- Etm 12 04 2383Document4 pagesEtm 12 04 2383mukhlis akmalPas encore d'évaluation
- Revised RRLDocument5 pagesRevised RRLJoshua ArcairaPas encore d'évaluation
- NIH Public Access: The Atopic March: Progression From Atopic Dermatitis To Allergic Rhinitis and AsthmaDocument16 pagesNIH Public Access: The Atopic March: Progression From Atopic Dermatitis To Allergic Rhinitis and Asthmasyak turPas encore d'évaluation
- Strachan Hygiene HypotheseDocument9 pagesStrachan Hygiene HypotheseRikko HudyonoPas encore d'évaluation
- En 14Document8 pagesEn 14buo_souzaPas encore d'évaluation
- Bab I Pendahuluan Latar Belakang: Universitas Sumatera UtaraDocument4 pagesBab I Pendahuluan Latar Belakang: Universitas Sumatera UtarakobexPas encore d'évaluation
- As Ma Pediatric ADocument6 pagesAs Ma Pediatric APatricia GuíoPas encore d'évaluation
- Diagnosis and Treatment of Chronic CoughD'EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoPas encore d'évaluation
- International Study ProtocolDocument9 pagesInternational Study ProtocolNicolas SaputraPas encore d'évaluation
- Growth Chest InfectionsDocument18 pagesGrowth Chest InfectionsjibianniePas encore d'évaluation
- Dermatitis AtopikDocument7 pagesDermatitis AtopiknyuwwchocolavaPas encore d'évaluation
- Nihms 661031 PDFDocument13 pagesNihms 661031 PDFryouchiimamuraPas encore d'évaluation
- Asthma: Signs and SymptomsDocument7 pagesAsthma: Signs and SymptomsPavitrra SubbramaniyamPas encore d'évaluation
- Dissertation ProposalDocument15 pagesDissertation ProposalJitesh SoniPas encore d'évaluation
- Review of Literature - Anusha BhandarkarDocument26 pagesReview of Literature - Anusha BhandarkarAnushaPas encore d'évaluation
- Asthma 2Document8 pagesAsthma 2Evangelist Stephen NziokaPas encore d'évaluation
- Smoking, Environmental Tobacco Smoke, and Aspirin-Exacerbated RespiratoryDocument6 pagesSmoking, Environmental Tobacco Smoke, and Aspirin-Exacerbated Respiratoryxiongmao2389Pas encore d'évaluation
- Internal Medicine Topic: Bronchial Asthma DR: Mousa Malkawy Lec #: 3 Date: 26-10-2009Document21 pagesInternal Medicine Topic: Bronchial Asthma DR: Mousa Malkawy Lec #: 3 Date: 26-10-2009Rashed ShatnawiPas encore d'évaluation
- New Developments in The Field of Allergy and AsthmaDocument4 pagesNew Developments in The Field of Allergy and Asthmameong_sweetPas encore d'évaluation
- Respiratory Viruses, Eosinophilia and Their Roles in Childhood AsthmaDocument11 pagesRespiratory Viruses, Eosinophilia and Their Roles in Childhood AsthmaeddcitoPas encore d'évaluation
- The Immunological Basis of The Hygiene HypothesisDocument19 pagesThe Immunological Basis of The Hygiene HypothesisRoxana Alarcón VásquezPas encore d'évaluation
- Bronchial Asthma Case StudyDocument35 pagesBronchial Asthma Case StudyMishiel Castillo100% (1)
- In The United StatesDocument15 pagesIn The United StatesirmaPas encore d'évaluation
- NIH Public Access: Comorbidity in Atopic DermatitisDocument16 pagesNIH Public Access: Comorbidity in Atopic DermatitiscrishPas encore d'évaluation
- Associations Between Environmental Heavy Metal Exposure and Childhood Asthma: A Population-Based StudyDocument11 pagesAssociations Between Environmental Heavy Metal Exposure and Childhood Asthma: A Population-Based StudyLeidy CarolinaPas encore d'évaluation
- Verstegen 2021 Dietary Fibers Effects Underlying MDocument32 pagesVerstegen 2021 Dietary Fibers Effects Underlying Mdr.martynchukPas encore d'évaluation
- Tosse Cronica em CriançasDocument17 pagesTosse Cronica em CriançasEdvaldo Pereira da Silva JúniorPas encore d'évaluation
- 2012 Health Disparity Asthma CourseDocument63 pages2012 Health Disparity Asthma CoursethomasPas encore d'évaluation
- 1991 - Darke, Guinan, Gold - Allergy and AsthmaDocument13 pages1991 - Darke, Guinan, Gold - Allergy and AsthmaPJ Chalet BookPas encore d'évaluation
- Review Article: Etiology and Risk Factors of Febrile Seizure - An UpdateDocument10 pagesReview Article: Etiology and Risk Factors of Febrile Seizure - An UpdateResty Rahmiliah RahimPas encore d'évaluation
- NIH Public Access: Rhinitis in Older AdultsDocument11 pagesNIH Public Access: Rhinitis in Older AdultsAnnisa RahmaniPas encore d'évaluation
- Current Strategies For Phenotyping and Managing Asthma in Preschool Children 2022Document8 pagesCurrent Strategies For Phenotyping and Managing Asthma in Preschool Children 2022Veronica Ofelia Morachimo GarcíaPas encore d'évaluation
- Jurnal DA 9Document8 pagesJurnal DA 9FIFIHPas encore d'évaluation
- BMC Pulmonary MedicineDocument15 pagesBMC Pulmonary MedicineAndra GulinPas encore d'évaluation
- Bronchial Asthma GuideDocument72 pagesBronchial Asthma GuidePrincewill SeiyefaPas encore d'évaluation
- No. 4Document18 pagesNo. 4FaridaHayatiPas encore d'évaluation
- Heart Kidney InteractionDocument11 pagesHeart Kidney InteractionMichael HostiadiPas encore d'évaluation
- Chronic Rinosinusitis in ChildrenDocument6 pagesChronic Rinosinusitis in ChildrenMichael HostiadiPas encore d'évaluation
- RdsDocument6 pagesRdsOlivia Valentine LekiPas encore d'évaluation
- The Role of Imaging in TheManagement of Cardiorenal SyndromeDocument7 pagesThe Role of Imaging in TheManagement of Cardiorenal SyndromeMichael HostiadiPas encore d'évaluation
- Med Surg Nasal PolypDocument10 pagesMed Surg Nasal PolypAsri HabsariPas encore d'évaluation
- Systemic Lupus Erythematosus (SLE)Document42 pagesSystemic Lupus Erythematosus (SLE)louradelPas encore d'évaluation
- Improving Prognosis Estimation in Patients With Heart FailureDocument11 pagesImproving Prognosis Estimation in Patients With Heart FailureMichael HostiadiPas encore d'évaluation
- Cardiorenal SyndromeDocument89 pagesCardiorenal SyndromeGabriyah HamzahPas encore d'évaluation
- Cardiac Resynchronization TherapyDocument6 pagesCardiac Resynchronization TherapyMichael HostiadiPas encore d'évaluation
- Clinical & Experimental Allergy: Vitamin D and Its Role in Allergic DiseaseDocument10 pagesClinical & Experimental Allergy: Vitamin D and Its Role in Allergic DiseaseMichael HostiadiPas encore d'évaluation
- Heart Kidney InteractionDocument11 pagesHeart Kidney InteractionMichael HostiadiPas encore d'évaluation
- Role of Vit D in Alergic RhinitisDocument5 pagesRole of Vit D in Alergic RhinitisMichael HostiadiPas encore d'évaluation
- Pathophysiology, Diagnosis, and Medical Management of Nonsurgical PatientsDocument14 pagesPathophysiology, Diagnosis, and Medical Management of Nonsurgical PatientsVanitha Ratha KrishnanPas encore d'évaluation
- Clinical Medicine: Vitamin D and The Development of Atopic EczemaDocument15 pagesClinical Medicine: Vitamin D and The Development of Atopic EczemaMichael HostiadiPas encore d'évaluation
- Senior Case Presentation 2Document38 pagesSenior Case Presentation 2Anonymous H8pAMbzrePas encore d'évaluation
- Acute Fungal Sinusitis Natural History and The Role of Frozen SectionDocument8 pagesAcute Fungal Sinusitis Natural History and The Role of Frozen SectionwitariPas encore d'évaluation
- Pathophysiology of Cluster HeadacheDocument13 pagesPathophysiology of Cluster HeadacheMichael HostiadiPas encore d'évaluation
- Allergic Rhinitis (NEJM 2015) PDFDocument8 pagesAllergic Rhinitis (NEJM 2015) PDFEduardo MenaPas encore d'évaluation
- Cluster Headache Workup - Approach ConsiderationsDocument3 pagesCluster Headache Workup - Approach ConsiderationsMichael HostiadiPas encore d'évaluation
- Path o PhysiologyDocument5 pagesPath o PhysiologyMichael HostiadiPas encore d'évaluation
- Acute TonsillitisDocument7 pagesAcute TonsillitisMichael HostiadiPas encore d'évaluation
- Cluster Headache - Background, Pathophysiology, EtiologyDocument5 pagesCluster Headache - Background, Pathophysiology, EtiologyMichael HostiadiPas encore d'évaluation
- Cluster Headache Clinical Presentation - History, Physical ExaminationDocument3 pagesCluster Headache Clinical Presentation - History, Physical ExaminationMichael HostiadiPas encore d'évaluation
- Path o PhysiologyDocument5 pagesPath o PhysiologyMichael HostiadiPas encore d'évaluation
- Pathophysiology of Cluster HeadacheDocument13 pagesPathophysiology of Cluster HeadacheMichael HostiadiPas encore d'évaluation
- Cluster PDFDocument15 pagesCluster PDFpurnawan29Pas encore d'évaluation
- TAREA 2 Marlin Rivas LDocument9 pagesTAREA 2 Marlin Rivas Lmarlin lobonPas encore d'évaluation
- Oregon COVID-19 Weekly Report (Published Oct. 21, 2020)Document33 pagesOregon COVID-19 Weekly Report (Published Oct. 21, 2020)KGW NewsPas encore d'évaluation
- Use of Convalescent Plasma in Hospitalized Patients With Covid-19 - Case SerieDocument12 pagesUse of Convalescent Plasma in Hospitalized Patients With Covid-19 - Case SeriesamuelPas encore d'évaluation
- Loa Loa and Onchocerca: Parasitic Filarial Worms Causing River BlindnessDocument28 pagesLoa Loa and Onchocerca: Parasitic Filarial Worms Causing River Blindnessbindu dhanapalPas encore d'évaluation
- Faktor-Faktor Yang Mempengaruhi Tuberculosis Multidrug Resistance (TB MDR)Document9 pagesFaktor-Faktor Yang Mempengaruhi Tuberculosis Multidrug Resistance (TB MDR)Dian RohmayantiPas encore d'évaluation
- Covid CertificateDocument3 pagesCovid CertificateanmolPas encore d'évaluation
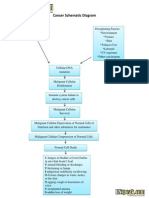
- Cancer Schematic DiagramDocument1 pageCancer Schematic DiagramCyrus De Asis100% (4)
- Pulse PressureDocument3 pagesPulse PressureYovie Anggara SaputraPas encore d'évaluation
- (Cuenca) Interview With The PHN NurseDocument2 pages(Cuenca) Interview With The PHN NurseTom CuencaPas encore d'évaluation
- Pathophysiology of AtherosclerosisDocument4 pagesPathophysiology of AtherosclerosisHardi AhmedPas encore d'évaluation
- AssignmentDocument14 pagesAssignmentAseer KhanPas encore d'évaluation
- What Is Coronavirus? The Different Types of CoronavirusesDocument9 pagesWhat Is Coronavirus? The Different Types of Coronavirusesashley bendanaPas encore d'évaluation
- Epidemiology of ObesityDocument32 pagesEpidemiology of ObesityamsabavanPas encore d'évaluation
- Infection Control in ICUDocument7 pagesInfection Control in ICUzenagit123456Pas encore d'évaluation
- Designated Medical Event Dme List enDocument3 pagesDesignated Medical Event Dme List enAmany HagagePas encore d'évaluation
- Behçet's SyndromeDocument12 pagesBehçet's SyndromeFernando Franco VargasPas encore d'évaluation
- Lung Cancer Treatment at Yashoda HospitalDocument4 pagesLung Cancer Treatment at Yashoda HospitalYashoda HospitalPas encore d'évaluation
- Case Study BlepharitisDocument12 pagesCase Study BlepharitisNorshahidah IedaPas encore d'évaluation
- Gendec - 2022-02-05T074422.847Document1 pageGendec - 2022-02-05T074422.847Robinson llanos ceraPas encore d'évaluation
- Dystonia: A ReviewDocument12 pagesDystonia: A ReviewMauro JacobsPas encore d'évaluation
- VSF Vet Pub Health Handbook South SudanDocument134 pagesVSF Vet Pub Health Handbook South Sudanabeza7007Pas encore d'évaluation
- Disease Essay Rubric - RetakeDocument2 pagesDisease Essay Rubric - Retakeapi-287032631Pas encore d'évaluation
- Surviving Sepsis Campaign Hour 1 BundleDocument5 pagesSurviving Sepsis Campaign Hour 1 BundleNadine Noelle AgraviadorPas encore d'évaluation
- Body Art Consent and Health Disclosure Form For Tattooing and PiercingDocument1 pageBody Art Consent and Health Disclosure Form For Tattooing and PiercingDanielPas encore d'évaluation
- World Doctors Alliance - Global Covid Report (October 2020)Document74 pagesWorld Doctors Alliance - Global Covid Report (October 2020)Floyd Reynolds100% (2)
- Pearls in Medicine For Students PDFDocument303 pagesPearls in Medicine For Students PDFGabriela Cordova Goicochea100% (2)
- Unconscious: By: Simranpreet KaurDocument12 pagesUnconscious: By: Simranpreet Kaurpreet kaurPas encore d'évaluation
- CDC 118387 DS1Document132 pagesCDC 118387 DS1Sina AyodejiPas encore d'évaluation
- B. Mahmoud - Salmonella - A Dangerous Foodborne Pathogen-Intech (2011)Document450 pagesB. Mahmoud - Salmonella - A Dangerous Foodborne Pathogen-Intech (2011)kiệt lêPas encore d'évaluation
- Ifugao State University Psychiatric Case StudyDocument6 pagesIfugao State University Psychiatric Case Studyfheb albertoPas encore d'évaluation