Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Gastroesophagea L of Reflux Disease (GERD)Document34 pagesGastroesophagea L of Reflux Disease (GERD)Alyda Choirunnissa SudiratnaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hyperlink IDocument1 pageHyperlink IAlyda Choirunnissa SudiratnaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Rheumatologi MANTAP TutorDocument36 pagesRheumatologi MANTAP TutorAlyda Choirunnissa SudiratnaPas encore d'évaluation
- Bu BD Uro Ortho Onko Mantap TutorDocument192 pagesBu BD Uro Ortho Onko Mantap TutorAlyda Choirunnissa Sudiratna50% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Tropmed MANTAP TutorDocument99 pagesTropmed MANTAP TutorAlyda Choirunnissa Sudiratna100% (1)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Incidence, Severity and Factors Related To Drug-Induced Keratoepitheliopathy With Glaucoma MedicationsDocument1 pageIncidence, Severity and Factors Related To Drug-Induced Keratoepitheliopathy With Glaucoma MedicationsAlyda Choirunnissa SudiratnaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- IPAQ Inggris PDFDocument4 pagesIPAQ Inggris PDFAlyda Choirunnissa SudiratnaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Maret Maret 3 Senin 4 Selasa 5 Rabu 6 Kamis 7 Jumat 8 Sabtu 9 Minggu Siang Pendi Icha Tommo Eka Afid Eitin Dhika Malam Afid Eitin Dhika Tammi Pendi Icha TommoDocument1 pageMaret Maret 3 Senin 4 Selasa 5 Rabu 6 Kamis 7 Jumat 8 Sabtu 9 Minggu Siang Pendi Icha Tommo Eka Afid Eitin Dhika Malam Afid Eitin Dhika Tammi Pendi Icha TommoAlyda Choirunnissa SudiratnaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Piriformis Syndrome: Hardi Adiyatma, Shahdevi Nandar KusumaDocument6 pagesPiriformis Syndrome: Hardi Adiyatma, Shahdevi Nandar Kusumaismael wandikboPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Presentation - Delight Bulb PDFDocument22 pagesPresentation - Delight Bulb PDFShiva KishorePas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Lesson 1 Chapter 9 ErosiondepositionDocument1 pageLesson 1 Chapter 9 Erosiondepositionapi-249320969Pas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Runyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechDocument28 pagesRunyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechThe New Vision50% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Bảng giá FLUKEDocument18 pagesBảng giá FLUKEVăn Long NguyênPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
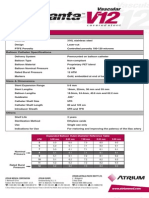
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiPas encore d'évaluation
- Technical Information: Range-Free Controller FA-M3 System Upgrade GuideDocument33 pagesTechnical Information: Range-Free Controller FA-M3 System Upgrade GuideAddaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Shandong Baoshida Cable Co, LTD.: Technical ParameterDocument3 pagesShandong Baoshida Cable Co, LTD.: Technical ParameterkmiqdPas encore d'évaluation
- Tugas 2-TRK Lanjut Kelompok 3 Andre-Arief-IstiaDocument18 pagesTugas 2-TRK Lanjut Kelompok 3 Andre-Arief-IstiaAndre Fahriz Perdana HarahapPas encore d'évaluation
- The FOA Reference For Fiber Optics - Fiber Optic TestingDocument19 pagesThe FOA Reference For Fiber Optics - Fiber Optic TestingvsalaiselvamPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Gypsum Plasterboard: National Standard of The People'S Republic of ChinaDocument15 pagesGypsum Plasterboard: National Standard of The People'S Republic of ChinaGarry100% (2)
- NF en Iso 5167-6-2019Document22 pagesNF en Iso 5167-6-2019Rem FgtPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Fully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019Document20 pagesFully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019lazareviciPas encore d'évaluation
- Rekomendasi AnimeDocument11 pagesRekomendasi Animeosvaldo manurungPas encore d'évaluation
- EN Manual Lenovo Ideapad S130-14igm S130-11igmDocument33 pagesEN Manual Lenovo Ideapad S130-14igm S130-11igmDolgoffPas encore d'évaluation
- MarbiehistoryDocument6 pagesMarbiehistoryMarbie DalanginPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Dual Op Amp and Voltage Reference Ap4310/ADocument12 pagesDual Op Amp and Voltage Reference Ap4310/AМихаил ЯненкоPas encore d'évaluation
- LG250CDocument2 pagesLG250CCarlosPas encore d'évaluation
- Bhil Tribal Mobilisation in AlirajpurDocument14 pagesBhil Tribal Mobilisation in Alirajpurrahul banerjeePas encore d'évaluation
- Ali Erdemir: Professional ExperienceDocument3 pagesAli Erdemir: Professional ExperienceDunkMePas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Elements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesDocument8 pagesElements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesSadman Shaid SaadPas encore d'évaluation
- Grade - 2 Subject - Mathematics Unit - Geometry Topic - Geometrical Shapes School - Army School Roorkee Prepared by Mrs. RanjanaDocument25 pagesGrade - 2 Subject - Mathematics Unit - Geometry Topic - Geometrical Shapes School - Army School Roorkee Prepared by Mrs. RanjanaPenke Mejado BelenPas encore d'évaluation
- Module 1 Notes The White Bird Reading The Image Painting Analysis PDFDocument4 pagesModule 1 Notes The White Bird Reading The Image Painting Analysis PDFMelbely Rose Apigo BaduaPas encore d'évaluation
- 2022 Audi e Tron 22Document318 pages2022 Audi e Tron 22Alejandro Alberto Robalino MendezPas encore d'évaluation
- Table Equivalent Schedule 40 Steel PipeDocument1 pageTable Equivalent Schedule 40 Steel PipeorisPas encore d'évaluation
- Case Studies of Transportation Public-Private Partnerships Around The WorldDocument158 pagesCase Studies of Transportation Public-Private Partnerships Around The WorldzhenhuaruiPas encore d'évaluation
- LET General Math ReviewerDocument7 pagesLET General Math ReviewerMarco Rhonel Eusebio100% (1)
- Scanner and Xcal Comperative Analysis v2Document22 pagesScanner and Xcal Comperative Analysis v2Ziya2009Pas encore d'évaluation
- Determination of Drop-Impact Resistance of Plastic BottlesDocument11 pagesDetermination of Drop-Impact Resistance of Plastic BottlesAndres BrañaPas encore d'évaluation
- Goldhofer FTV 850 BrochureDocument2 pagesGoldhofer FTV 850 BrochureMauroPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)