Vous aimerez peut-être aussi
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Extended Report: ObjectivesDocument8 pagesExtended Report: ObjectivesIuliana NitaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- PRISMA P ChecklistDocument2 pagesPRISMA P ChecklistAssem GamalPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- BMJ g7647 FullDocument25 pagesBMJ g7647 FullIuliana NitaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Boards' Fodder: AlopeciaDocument2 pagesBoards' Fodder: AlopeciaIuliana NitaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Mabs0401 0110Document10 pagesMabs0401 0110Iuliana NitaPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Mabs0401 0110Document10 pagesMabs0401 0110Iuliana NitaPas encore d'évaluation
- Therapeutic Monoclonal Antibodies and The Need For Targeted Pharmacovigilance in IndiaDocument5 pagesTherapeutic Monoclonal Antibodies and The Need For Targeted Pharmacovigilance in IndiaIuliana NitaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Singh 2011Document84 pagesSingh 2011Iuliana NitaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Kew 442Document9 pagesKew 442Iuliana NitaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Icmje Recommendations PDFDocument17 pagesIcmje Recommendations PDFFebyan AbotPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- Guidelines of Care For The Management of Acne VulgarisDocument53 pagesGuidelines of Care For The Management of Acne VulgarisIuliana NitaPas encore d'évaluation
- Stevenson 2017Document13 pagesStevenson 2017Iuliana NitaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Factors in Uencing The Immunogenicity of Therapeutic ProteinsDocument7 pagesFactors in Uencing The Immunogenicity of Therapeutic ProteinsIuliana NitaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Stevenson 2017Document13 pagesStevenson 2017Iuliana NitaPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Am18 Poster Exhibits GuidelinesDocument3 pagesAm18 Poster Exhibits GuidelinesIuliana NitaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Trends in Sunscreen Recommendation Among US Physicians: Original InvestigationDocument5 pagesTrends in Sunscreen Recommendation Among US Physicians: Original InvestigationIuliana NitaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- ICMJE Form PDFDocument1 pageICMJE Form PDFsanjayb1008491Pas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Patient CommunicationDocument16 pagesPatient CommunicationIuliana NitaPas encore d'évaluation
- How To Get PublishedDocument2 pagesHow To Get PublishedIuliana NitaPas encore d'évaluation
- SwichDocument6 pagesSwichIuliana NitaPas encore d'évaluation
- Jcad 10 3 s1 8Document8 pagesJcad 10 3 s1 8Iuliana NitaPas encore d'évaluation
- PRISMA 2009 Checklist: An AnalysisDocument2 pagesPRISMA 2009 Checklist: An AnalysisFiŗåš ÀßßâşPas encore d'évaluation
- Communication and Active ListeningDocument18 pagesCommunication and Active ListeningIuliana NitaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Doyle 2013Document12 pagesDoyle 2013Iuliana NitaPas encore d'évaluation
- Ultrasound Study of Entheses in Psoriasis Patients With or Without Musculoskeletal Symptoms A Prospective StudyDocument5 pagesUltrasound Study of Entheses in Psoriasis Patients With or Without Musculoskeletal Symptoms A Prospective StudyIuliana NitaPas encore d'évaluation
- On Diagnostic Rationality: Bad News, Good News, and The Symptom ResidueDocument37 pagesOn Diagnostic Rationality: Bad News, Good News, and The Symptom ResidueIuliana NitaPas encore d'évaluation
- The Salford Psoriasis Index An Holistic Measure of Psoriasis SeverityDocument5 pagesThe Salford Psoriasis Index An Holistic Measure of Psoriasis SeverityIuliana NitaPas encore d'évaluation
- The Relationship Between Nail - and Distal Phalangeal BoneDocument3 pagesThe Relationship Between Nail - and Distal Phalangeal BoneIuliana NitaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
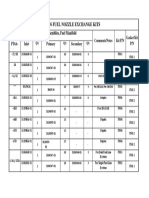
- Pt6 Fuel Nozzle Exchange Kits: Adapter Assemblies, Fuel ManifoldDocument1 pagePt6 Fuel Nozzle Exchange Kits: Adapter Assemblies, Fuel ManifoldBerchPas encore d'évaluation
- Symmetry & Crystal StructuresDocument37 pagesSymmetry & Crystal StructuresNurnajihah Sukimi JiehaPas encore d'évaluation
- Bomba Electrica 1500gpm 300HP (Medidas)Document1 pageBomba Electrica 1500gpm 300HP (Medidas)Fire ChilePas encore d'évaluation
- TDFC Global Engineering Solutions CompanyDocument189 pagesTDFC Global Engineering Solutions CompanyplanningPas encore d'évaluation
- Thermal Shock Resistant Neoceram Glass-CeramicDocument2 pagesThermal Shock Resistant Neoceram Glass-CeramicAmândio PintoPas encore d'évaluation
- Damper mechanism details for Atlas Copco rock drills under 40 charactersDocument27 pagesDamper mechanism details for Atlas Copco rock drills under 40 characterssalvador341100% (2)
- Projects Oil and Gas BrochureDocument20 pagesProjects Oil and Gas BrochureRussel John RamosPas encore d'évaluation
- Flat Roof 1Document10 pagesFlat Roof 1agent206Pas encore d'évaluation
- Chilled Water Pipe Insulation Method StatementDocument2 pagesChilled Water Pipe Insulation Method StatementGündoğdu Akın75% (4)
- Master Plan 2021Document172 pagesMaster Plan 2021Rajnish MishraPas encore d'évaluation
- SGMF Hose BunkeringDocument15 pagesSGMF Hose BunkeringFilipPas encore d'évaluation
- 4 - ch01 - SQ - E: Solutions MarksDocument37 pages4 - ch01 - SQ - E: Solutions Marks5A35 YIP HOI PAKPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Overhead Phil MC KeownDocument30 pagesOverhead Phil MC KeownAditya AolePas encore d'évaluation
- EDM Technologies: Electrical Discharge Machining ServicesDocument8 pagesEDM Technologies: Electrical Discharge Machining Servicesfarahin_selamatPas encore d'évaluation
- Mechanics - Fluid Dynamics: K. Suresh Senanayake 1Document2 pagesMechanics - Fluid Dynamics: K. Suresh Senanayake 1mangsureshPas encore d'évaluation
- Energy Manipulation and MeditationDocument6 pagesEnergy Manipulation and Meditationapi-246292178100% (1)
- SUPER PPTPPTDocument15 pagesSUPER PPTPPTsrinuPas encore d'évaluation
- System Sensor 2WTR-B Data SheetDocument2 pagesSystem Sensor 2WTR-B Data SheetJMAC SupplyPas encore d'évaluation
- ECU MS 3 Sport GT3 Cup Manual Setup GuideDocument26 pagesECU MS 3 Sport GT3 Cup Manual Setup GuideAngel LópezPas encore d'évaluation
- RECYCLED ASPHALTDocument27 pagesRECYCLED ASPHALTwillypraviantoPas encore d'évaluation
- 262 Controlled Switching of HVAC Circuit Breaker PDFDocument34 pages262 Controlled Switching of HVAC Circuit Breaker PDFepriPas encore d'évaluation
- Kiln Audit Heat Balance Tool - Data Entry Sheet 4 - CoolerDocument1 pageKiln Audit Heat Balance Tool - Data Entry Sheet 4 - CoolerMohamed SelimPas encore d'évaluation
- 42SL80 TrainingDocument93 pages42SL80 Trainingvmalvica67% (3)
- Method of Lighting CalculationsDocument3 pagesMethod of Lighting CalculationsSpencer Josh RegedorPas encore d'évaluation
- Krff302ess01 Tech Sheet - w10787422 - Rev CDocument10 pagesKrff302ess01 Tech Sheet - w10787422 - Rev CJesikaGomezSaavedraPas encore d'évaluation
- Test 48Document9 pagesTest 48Thị VyPas encore d'évaluation
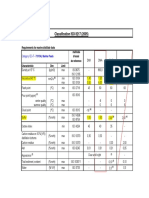
- Classification ISO 8217 (2005)Document5 pagesClassification ISO 8217 (2005)Salah JallaliPas encore d'évaluation
- 2013 Renault ZOE PresskitDocument34 pages2013 Renault ZOE PresskitDidelisPas encore d'évaluation
- Dolphin by EnOcean enDocument16 pagesDolphin by EnOcean en刘嘉伟Pas encore d'évaluation
- CH 1Document13 pagesCH 1badgujar_bandhuPas encore d'évaluation
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (13)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)