Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
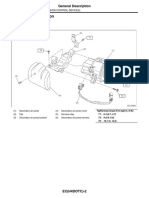
- Emission+Control+ (Aux +Emission+Control+Devices) + (H4DOTC)Document27 pagesEmission+Control+ (Aux +Emission+Control+Devices) + (H4DOTC)Marcelo BedoyaPas encore d'évaluation
- Valadi - Guillain-Barré SyndromeDocument5 pagesValadi - Guillain-Barré SyndromeMarcelo BedoyaPas encore d'évaluation
- Ubogu - Inflammatory NeuropathiesDocument24 pagesUbogu - Inflammatory NeuropathiesMarcelo BedoyaPas encore d'évaluation
- 2014 Fokke GBS Brighton Brain 2014Document11 pages2014 Fokke GBS Brighton Brain 2014Hikmat SatriaPas encore d'évaluation
- Asbury - Assesment of Current Diagnostic Criteria For GBSDocument4 pagesAsbury - Assesment of Current Diagnostic Criteria For GBSMarcelo BedoyaPas encore d'évaluation
- Pokemon: Opening Theme: XylophoneDocument17 pagesPokemon: Opening Theme: XylophoneMarcelo BedoyaPas encore d'évaluation
- +09 US Geological Survey - Mineral Commodity Summaries 2016Document205 pages+09 US Geological Survey - Mineral Commodity Summaries 2016Marcelo BedoyaPas encore d'évaluation
- 13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentDocument21 pages13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentMarcelo BedoyaPas encore d'évaluation
- CG54 MigratedDocument34 pagesCG54 MigratedMarcelo BedoyaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Oxford Specialist Handbooks Addiction Medicine 2009 PDFDocument492 pagesOxford Specialist Handbooks Addiction Medicine 2009 PDFMahmoud Hassan100% (1)
- American Academy of Pediatrics: ABBREVIATION. PICU, Pediatric Intensive Care UnitDocument3 pagesAmerican Academy of Pediatrics: ABBREVIATION. PICU, Pediatric Intensive Care UnitdoctorsamitPas encore d'évaluation
- Emergency Poisoning FinalDocument81 pagesEmergency Poisoning FinalMohammed Gazo100% (2)
- SIADH, DI and Cerebral Salt Wasting: Karim Rafaat, MDDocument54 pagesSIADH, DI and Cerebral Salt Wasting: Karim Rafaat, MDMahendra PrasetyoPas encore d'évaluation
- Lacosamide TreatmentDocument13 pagesLacosamide TreatmentawinsyPas encore d'évaluation
- 2014 - SMFM - Society For Maternal-Fetal Medicine (SMFM) Special Report, The Maternal-Fetal Medicine Subspecialists' Role Within A Health Care SystemDocument10 pages2014 - SMFM - Society For Maternal-Fetal Medicine (SMFM) Special Report, The Maternal-Fetal Medicine Subspecialists' Role Within A Health Care SystemjrPas encore d'évaluation
- Vac Lok Cushions GuideDocument9 pagesVac Lok Cushions GuideYS TangPas encore d'évaluation
- AcneDocument38 pagesAcneSavanna ChambersPas encore d'évaluation
- Ch1 Perspective of Pediatric NursingDocument110 pagesCh1 Perspective of Pediatric Nursing9cptb4x7sxPas encore d'évaluation
- Retrocolic Isoperistaltic Gastrojejunostomy As An Alternative To Kimura's Duodenoduodenostomy in Low and Very Low Birth Weight Babies of Duodenal AtresiaDocument4 pagesRetrocolic Isoperistaltic Gastrojejunostomy As An Alternative To Kimura's Duodenoduodenostomy in Low and Very Low Birth Weight Babies of Duodenal AtresiaBeni BolngPas encore d'évaluation
- Network HospitalsDocument92 pagesNetwork Hospitalsvengatraj880% (1)
- Border Molding & Vent HolesDocument4 pagesBorder Molding & Vent HolesGina Kissey100% (1)
- Pregnancy CKDDocument6 pagesPregnancy CKDRajiv MedankiPas encore d'évaluation
- Dafpus Ror BDHDocument3 pagesDafpus Ror BDHSamuel Hananiel RoryPas encore d'évaluation
- BDS-Batch 11-Module 1 - CA - Anatomy Question BankDocument2 pagesBDS-Batch 11-Module 1 - CA - Anatomy Question BankcheckmatePas encore d'évaluation
- Abg Analysis ReviewerDocument21 pagesAbg Analysis ReviewerAyiessa_AJPas encore d'évaluation
- Osteopathy InfographicDocument1 pageOsteopathy Infographicapi-614436724Pas encore d'évaluation
- Important Pediatrics SyndromesDocument11 pagesImportant Pediatrics SyndromesYogeshRavalPas encore d'évaluation
- PEDIA Review TransesDocument12 pagesPEDIA Review TransesanonymousPas encore d'évaluation
- DR Writing 001 OET Practice Letter by PASS OETDocument3 pagesDR Writing 001 OET Practice Letter by PASS OETmuthu18933% (6)
- Winning Piece FeatureDocument9 pagesWinning Piece FeatureHowardPas encore d'évaluation
- Strengths and Weaknesses of Midwifery Care From TheDocument9 pagesStrengths and Weaknesses of Midwifery Care From TheDita Rahmaika APas encore d'évaluation
- Randomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseDocument9 pagesRandomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseTommy WidjayaPas encore d'évaluation
- Ectopic Pregnancy StudyDay Course FacultyDocument1 pageEctopic Pregnancy StudyDay Course FacultyWAGS CommitteePas encore d'évaluation
- Information Sheet For Applicants For Employers of Indonesia Candidates For "Kangoshi"Document11 pagesInformation Sheet For Applicants For Employers of Indonesia Candidates For "Kangoshi"bnp2tkidotgodotidPas encore d'évaluation
- Nevada Sagebrush Archives For 03152016Document10 pagesNevada Sagebrush Archives For 03152016The Nevada SagebrushPas encore d'évaluation
- Delayed Replantation of An Avulsed Maxillary Premolar With Open Apex: A 24 Months Follow-Up Case ReportDocument5 pagesDelayed Replantation of An Avulsed Maxillary Premolar With Open Apex: A 24 Months Follow-Up Case ReportDiego Andres Hincapie HerreraPas encore d'évaluation
- Clinical Guide To Use VictozaDocument2 pagesClinical Guide To Use VictozaHarkeeratPas encore d'évaluation
- Ehra Position Paper: Europace (2018) 20, 1719-1720 Doi:10.1093/europace/eux380Document35 pagesEhra Position Paper: Europace (2018) 20, 1719-1720 Doi:10.1093/europace/eux380Karen OezauPas encore d'évaluation
- Mannitol Clinical PREADocument9 pagesMannitol Clinical PREAjoelrequenaPas encore d'évaluation