Vous aimerez peut-être aussi
- Parade OK 3 07 June 2017Document9 pagesParade OK 3 07 June 2017Dini NanamiPas encore d'évaluation
- Ocular Trauma SlideDocument49 pagesOcular Trauma SlideRizky FajriPas encore d'évaluation
- Mapping RabuDocument6 pagesMapping RabuDini NanamiPas encore d'évaluation
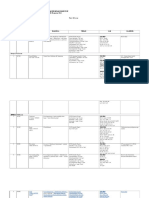
- Rekap Pasien Bedah Digestive Minggu, 13 November 2016: Nama Dokter MudaDocument6 pagesRekap Pasien Bedah Digestive Minggu, 13 November 2016: Nama Dokter MudaDini NanamiPas encore d'évaluation
- 29.full BolehDocument7 pages29.full BolehDini NanamiPas encore d'évaluation
- Theron Et Al 2011Document9 pagesTheron Et Al 2011Dini NanamiPas encore d'évaluation
- Jurnal TB 1Document18 pagesJurnal TB 1Dini NanamiPas encore d'évaluation
- Soal Uts Lp3iDocument1 pageSoal Uts Lp3iDini NanamiPas encore d'évaluation
- Rekap Pasien Bedah Digestive Selasa, 08 November 2016: Nama Dokter MudaDocument6 pagesRekap Pasien Bedah Digestive Selasa, 08 November 2016: Nama Dokter MudaDini NanamiPas encore d'évaluation
- ABC of DermatologyDocument149 pagesABC of DermatologyAndreea Alexandru100% (14)
- No TBDocument8 pagesNo TBDini NanamiPas encore d'évaluation
- No Agak TBDocument9 pagesNo Agak TBDini NanamiPas encore d'évaluation
- Tuberculosis 140515184439 Phpapp01Document47 pagesTuberculosis 140515184439 Phpapp01Veronica Wong Huey ShinPas encore d'évaluation
- Tuberculosis 140515184439 Phpapp01Document47 pagesTuberculosis 140515184439 Phpapp01Veronica Wong Huey ShinPas encore d'évaluation
- Treatment of Complicated Parapneumonic Pleural Medscimonit 2012Document7 pagesTreatment of Complicated Parapneumonic Pleural Medscimonit 2012DianaWilderPas encore d'évaluation
- Jurnal TB 2Document6 pagesJurnal TB 2Dini NanamiPas encore d'évaluation
- Pone 0149258Document16 pagesPone 0149258Dini NanamiPas encore d'évaluation
- Jurnal 3Document11 pagesJurnal 3Dini NanamiPas encore d'évaluation
- Jurnal TB 1Document18 pagesJurnal TB 1Dini NanamiPas encore d'évaluation
- Slide Dini JurnalDocument22 pagesSlide Dini JurnalDini NanamiPas encore d'évaluation
- Slide Dini JurnalDocument34 pagesSlide Dini JurnalDini NanamiPas encore d'évaluation
- Theron Et Al 2011Document9 pagesTheron Et Al 2011Dini NanamiPas encore d'évaluation
- Radiological Features of BronchiectasisDocument24 pagesRadiological Features of BronchiectasisOxana TurcuPas encore d'évaluation
- The God Factor - The Role of Religious Involvement On DepressionDocument122 pagesThe God Factor - The Role of Religious Involvement On DepressionDini NanamiPas encore d'évaluation
- Chronic Diarrhea GuideDocument14 pagesChronic Diarrhea GuideDini NanamiPas encore d'évaluation
- Art:10.1007/s00431 007 0419 XDocument8 pagesArt:10.1007/s00431 007 0419 XDini NanamiPas encore d'évaluation
- Functional Diarrhea in Toddlers (Chronic Nonspeci Fi C Diarrhea)Document4 pagesFunctional Diarrhea in Toddlers (Chronic Nonspeci Fi C Diarrhea)Dini NanamiPas encore d'évaluation
- DissertationDocument228 pagesDissertationDini NanamiPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Ethical Issues in Nursing Research:: Deontological PerspectiveDocument11 pagesEthical Issues in Nursing Research:: Deontological PerspectiveJM JavienPas encore d'évaluation
- Multi-Specialty Hospital: Ram Sharada Healthcare Pvt. LTDDocument48 pagesMulti-Specialty Hospital: Ram Sharada Healthcare Pvt. LTDsubhash goelPas encore d'évaluation
- William Obstetric 24th Study GuideDocument447 pagesWilliam Obstetric 24th Study GuideNizam Kunong100% (2)
- Memo No. 2022-59 - Submission of Updated PHIC and PRC License of Medical SpecialistsDocument8 pagesMemo No. 2022-59 - Submission of Updated PHIC and PRC License of Medical SpecialistsPaul Rizel LedesmaPas encore d'évaluation
- Effectiveness of Information, Education and Communication Package On Knowledge On Developmental Care Among Mothers of Low Birth Weight BabiesDocument12 pagesEffectiveness of Information, Education and Communication Package On Knowledge On Developmental Care Among Mothers of Low Birth Weight Babiesiaset123Pas encore d'évaluation
- 1) Community PharmacyDocument17 pages1) Community PharmacyDr. Zirwa AsimPas encore d'évaluation
- 75 5056am0703 614 623Document10 pages75 5056am0703 614 623Rizkhy WahyuPas encore d'évaluation
- A Brief History of EndodonticsDocument5 pagesA Brief History of EndodonticsDidi PascalauPas encore d'évaluation
- A Multidisciplinary Care Map For A Woman in Preterm Labor LazaletaDocument3 pagesA Multidisciplinary Care Map For A Woman in Preterm Labor Lazaletablythe RiveroPas encore d'évaluation
- The Generics ActDocument19 pagesThe Generics ActCJ Halasan100% (1)
- Small But Intriguing The Unfolding Story of Homeopathic Medicine PDFDocument7 pagesSmall But Intriguing The Unfolding Story of Homeopathic Medicine PDFweb3351Pas encore d'évaluation
- End of Life Summit FICA References PDFDocument2 pagesEnd of Life Summit FICA References PDFTejas PatilPas encore d'évaluation
- Emp Master 09042015Document80 pagesEmp Master 09042015Joe SalisPas encore d'évaluation
- Teaching Faculty For Allied Health Sciences - 2021Document9 pagesTeaching Faculty For Allied Health Sciences - 2021jamoonPas encore d'évaluation
- Hepatitis B InfectionDocument8 pagesHepatitis B Infectionto van quyenPas encore d'évaluation
- Research On Prison HealthcDocument87 pagesResearch On Prison HealthcptsievccdPas encore d'évaluation
- Rapid Is 2015Document11 pagesRapid Is 2015José Cunha CoutinhoPas encore d'évaluation
- Contoh Format Laporan SoapDocument5 pagesContoh Format Laporan SoapAchmad Triwidodo AmoePas encore d'évaluation
- Ayushman Bharat PMJAY Branding GuidelinesDocument10 pagesAyushman Bharat PMJAY Branding GuidelinesalkaPas encore d'évaluation
- Routine Health Information System: by Atsede Mazengia (BSC, MPH) Uog-2022Document374 pagesRoutine Health Information System: by Atsede Mazengia (BSC, MPH) Uog-2022Birhanu GirmaPas encore d'évaluation
- Children's Services Job DescriptionDocument11 pagesChildren's Services Job DescriptionMuhammad Dian Luthfy LubisPas encore d'évaluation
- Final Report On The Audit of Peace Corps Panama IG-18-01-ADocument32 pagesFinal Report On The Audit of Peace Corps Panama IG-18-01-AAccessible Journal Media: Peace Corps DocumentsPas encore d'évaluation
- Student'S Health Information Form: (E.g. Frequency, Extent, Duration, Ongoing Therapy, Etc.)Document2 pagesStudent'S Health Information Form: (E.g. Frequency, Extent, Duration, Ongoing Therapy, Etc.)Susan Loida SorianoPas encore d'évaluation
- Petrosea Klinik Medical Services AgreementDocument29 pagesPetrosea Klinik Medical Services AgreementChaqhim YvciPas encore d'évaluation
- Rebekah Antoine: WORK EXPERIENCEDocument6 pagesRebekah Antoine: WORK EXPERIENCEapi-416398178Pas encore d'évaluation
- Ess 7Document4 pagesEss 7api-582020074Pas encore d'évaluation
- B.Sc. Handbook 2018-21Document59 pagesB.Sc. Handbook 2018-21Manisha NishaPas encore d'évaluation
- ASHP Guidelines On PNTCDocument10 pagesASHP Guidelines On PNTCNosheen KhizarPas encore d'évaluation
- NEW m1m2 Reporting FormDocument24 pagesNEW m1m2 Reporting FormDeyeck Verga100% (8)
- IRMNCH Nutrition ServicesDocument26 pagesIRMNCH Nutrition ServicesAftab AlmaniPas encore d'évaluation