Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- GlycolipidsDocument1 pageGlycolipidsRuchini EdiriweeraPas encore d'évaluation
- Lipids Function and StructureDocument58 pagesLipids Function and StructureTeddy K KunongPas encore d'évaluation
- Golnic Lipidai Fingernails 000029915Document9 pagesGolnic Lipidai Fingernails 000029915Vita BūdvytėPas encore d'évaluation
- Chapter 3.1 - LipidsDocument35 pagesChapter 3.1 - LipidsDazell VarronPas encore d'évaluation
- GlycerophospholipidsDocument2 pagesGlycerophospholipidsHANNA CASANDRA GARCIAPas encore d'évaluation
- Biosint de LipDocument24 pagesBiosint de LipdborghiPas encore d'évaluation
- (by-Motohashi,-Noboru) Occurrences,-Structure,-Bio-2638182Document220 pages(by-Motohashi,-Noboru) Occurrences,-Structure,-Bio-2638182Kotoch HaraPas encore d'évaluation
- M1 Lesson 1: Introduction To Biochemistry Part 3Document12 pagesM1 Lesson 1: Introduction To Biochemistry Part 3CHARLES RONALD GENATOPas encore d'évaluation
- Sphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeDocument12 pagesSphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeUzac BenuPas encore d'évaluation
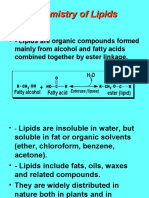
- Chemistry of LipidsDocument19 pagesChemistry of LipidsJohn Rick Orine100% (1)
- Lipids Function and StructureDocument60 pagesLipids Function and StructureIndra GunawanPas encore d'évaluation
- Understanding Lipids: Definition, Classification and Biological ImportanceDocument88 pagesUnderstanding Lipids: Definition, Classification and Biological ImportanceDanielle Anne Zamora-Matillosa LambanPas encore d'évaluation
- Lipids Chemistry GuideDocument88 pagesLipids Chemistry GuideKesha Marie TalloPas encore d'évaluation
- SAS For Biochemistry BIO 024 Module 2 2Document38 pagesSAS For Biochemistry BIO 024 Module 2 2syriljen mamolangPas encore d'évaluation
- Phospholipid MetabolismDocument32 pagesPhospholipid MetabolismOnSolomonPas encore d'évaluation
- Lipids Structure and Classification GuideDocument83 pagesLipids Structure and Classification GuideGOT7 ł IGOT7 TRUSTPas encore d'évaluation
- Lipids NotesDocument5 pagesLipids NotesnofacejackPas encore d'évaluation
- BIOMOLECULESDocument54 pagesBIOMOLECULESTanmayPas encore d'évaluation
- Lipids Function and StructureDocument60 pagesLipids Function and StructureDifa Kartika BakriePas encore d'évaluation
- Chemistry of LipidsDocument92 pagesChemistry of LipidsSumit Tated100% (2)
- LipidDocument31 pagesLipidصالح مقالحPas encore d'évaluation
- 17.6 SphingolipidsDocument15 pages17.6 SphingolipidsGerald Angelo DeguinioPas encore d'évaluation
- Understanding Lipid ChemistryDocument116 pagesUnderstanding Lipid ChemistryElfitri KusumawardhaniPas encore d'évaluation
- Understanding Glycolipids: Cerebrosides, Gangliosides and their TypesDocument103 pagesUnderstanding Glycolipids: Cerebrosides, Gangliosides and their TypesRahul AchariPas encore d'évaluation
- General Biochemistry (BCH 201) Section: Chemistry of Lipids Course OutlineDocument28 pagesGeneral Biochemistry (BCH 201) Section: Chemistry of Lipids Course OutlineOjo OluwafunkePas encore d'évaluation
- Structure and Function of LipidsDocument8 pagesStructure and Function of Lipidsalphius_mendoza50% (2)