Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Proceedings 6th Violence in Clinical Psychiatry 2009Document388 pagesProceedings 6th Violence in Clinical Psychiatry 2009yodoid100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Homelessness and Mental HealthDocument343 pagesHomelessness and Mental Healthiuhuh100% (1)
- Moral Panics, Mental Illness Stigma, and The Deinstitutionalization Movement in American Popular Culture PDFDocument194 pagesMoral Panics, Mental Illness Stigma, and The Deinstitutionalization Movement in American Popular Culture PDFCaroline HollandPas encore d'évaluation
- Kpds 2005 Kasım SonbaharDocument16 pagesKpds 2005 Kasım SonbaharDr. Hikmet ŞahinerPas encore d'évaluation
- Chapter 1 - Foundations of Psychiatric - Mental Health NursingDocument5 pagesChapter 1 - Foundations of Psychiatric - Mental Health NursingCatia Fernandes100% (2)
- Interior Design - Definition, Practice and Its Necessity: Architect/Enp Marie Grace A. PatadlasDocument93 pagesInterior Design - Definition, Practice and Its Necessity: Architect/Enp Marie Grace A. PatadlasCJ OngPas encore d'évaluation
- Madness - A Very Short Introduction-ReviewDocument2 pagesMadness - A Very Short Introduction-Reviewismaeel_ghPas encore d'évaluation
- Carla Yanni The Architecture of Madness Insane Asylums in The United States Architecture Landscape and Amer Culture 2007Document206 pagesCarla Yanni The Architecture of Madness Insane Asylums in The United States Architecture Landscape and Amer Culture 2007Joana Melo Resende100% (3)
- Canadian Standards For Psychiatric Mental Health NursingDocument28 pagesCanadian Standards For Psychiatric Mental Health NursingJoannePas encore d'évaluation
- Mad in AmericaDocument13 pagesMad in AmericaSadia AshrafPas encore d'évaluation
- Stigma Paper enDocument20 pagesStigma Paper enkartikaffPas encore d'évaluation
- City London MapDocument1 pageCity London MapkartikaffPas encore d'évaluation
- 1 Advocacy WEB 07Document72 pages1 Advocacy WEB 07kartikaffPas encore d'évaluation
- Westminster MapDocument1 pageWestminster MapkartikaffPas encore d'évaluation
- Language LevelsDocument1 pageLanguage LevelsProfesoraELEPas encore d'évaluation
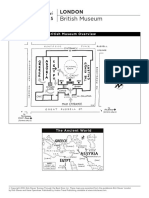
- British Museum MapDocument2 pagesBritish Museum MapkartikaffPas encore d'évaluation
- British Library MapDocument1 pageBritish Library MapkartikaffPas encore d'évaluation
- National Mental Health ProgramDocument14 pagesNational Mental Health ProgramDr. Jayesh Patidar100% (1)
- PSYCHIATRY (Edited by Prof. Gavenko V.L.)Document388 pagesPSYCHIATRY (Edited by Prof. Gavenko V.L.)NIDHIL SYAMPas encore d'évaluation
- Highlighting Successes and Challenges of The Mental Health System in Tunisia An Overview of Services Facilities and Human ResourcesDocument10 pagesHighlighting Successes and Challenges of The Mental Health System in Tunisia An Overview of Services Facilities and Human ResourcesMahmoud KamounPas encore d'évaluation
- 260404the Salpetriere in The Age of CharcotDocument30 pages260404the Salpetriere in The Age of CharcotdadaaucoeurPas encore d'évaluation
- Best Information BookDocument178 pagesBest Information BookMubashar HussainPas encore d'évaluation
- Community Psychiatric Services in Malaysia Where Do We Go From Here DR Abd KadirDocument3 pagesCommunity Psychiatric Services in Malaysia Where Do We Go From Here DR Abd KadiralyatasyaPas encore d'évaluation
- Deinstitutionalization 2Document9 pagesDeinstitutionalization 2api-297149827Pas encore d'évaluation
- No Room at The Inn-2012Document28 pagesNo Room at The Inn-2012Treatment Advocacy CenterPas encore d'évaluation
- The Karnataka Prisons Act, 1963Document20 pagesThe Karnataka Prisons Act, 1963Sridhara babu. N - ಶ್ರೀಧರ ಬಾಬು. ಎನ್Pas encore d'évaluation
- SynopsisDocument6 pagesSynopsishareniPas encore d'évaluation
- Changing Focus of CareDocument38 pagesChanging Focus of CareManoj BalaPas encore d'évaluation
- Chapter 18Document23 pagesChapter 18M SyafiPas encore d'évaluation
- Evolution of Mental Health CareDocument78 pagesEvolution of Mental Health CareAttaullah khan100% (1)
- Spaced-Out in Saskatchewan - Modernism, Anti-Psychiatry, and DeinstitutionalizationDocument29 pagesSpaced-Out in Saskatchewan - Modernism, Anti-Psychiatry, and DeinstitutionalizationAmritha V RaoPas encore d'évaluation
- Psychology Exam Chapter 1Document29 pagesPsychology Exam Chapter 1Besim HasangjekajPas encore d'évaluation
- Mental - IllnessDocument15 pagesMental - IllnessAhmad DawudPas encore d'évaluation
- Pabasari Ginige: January 20 THDocument28 pagesPabasari Ginige: January 20 THJagath NissankaPas encore d'évaluation
- Mnemonic SDocument131 pagesMnemonic SVicky RajoraPas encore d'évaluation
- Title 25 Chapter 134: Psychiatric HospDocument172 pagesTitle 25 Chapter 134: Psychiatric HosposcartxnPas encore d'évaluation
- Hist Madness SyllabusDocument7 pagesHist Madness Syllabusgae24341Pas encore d'évaluation