Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Case 3Document8 pagesCase 3Roberto RamosPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Soap RoutineDocument3 pagesSoap RoutineRoberto Ramos100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- History: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasDocument9 pagesHistory: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasRoberto RamosPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Paciente 3Document80 pagesPaciente 3Roberto RamosPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Universidad Puerto Rico Manual 1415Document161 pagesUniversidad Puerto Rico Manual 1415Roberto RamosPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- DR - Umpierrere2012 2013 4Document70 pagesDR - Umpierrere2012 2013 4Roberto RamosPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
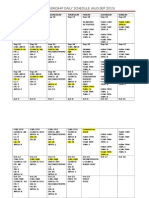
- Ob-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Document3 pagesOb-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Roberto RamosPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- HTTPDocument1 pageHTTPRoberto RamosPas encore d'évaluation
- Modified Diploma Logbook 2011 2012Document109 pagesModified Diploma Logbook 2011 2012Khalid ElmasryPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Peace Corps Mefloquine Policy March 2015 Letter To DirectorDocument7 pagesPeace Corps Mefloquine Policy March 2015 Letter To DirectorAccessible Journal Media: Peace Corps DocumentsPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- AnencephalyDocument11 pagesAnencephalyAnironOrionPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Gingivita Din Ciclul MenstrualDocument10 pagesGingivita Din Ciclul MenstrualRamonaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Novartis Vigamox-Product (API+excipient)Document15 pagesNovartis Vigamox-Product (API+excipient)auliana khusniatiPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- National Strategic Plan 2017-25Document144 pagesNational Strategic Plan 2017-25SPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Group B-2 Operation Management ProjectDocument17 pagesGroup B-2 Operation Management Projectanksri07Pas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Sun MediMax TableDocument1 pageSun MediMax TableKhairul RafiziPas encore d'évaluation
- Substance UseDocument3 pagesSubstance UseAlbert SamantePas encore d'évaluation
- Medication Administration Errors: Understanding The IssuesDocument9 pagesMedication Administration Errors: Understanding The IssuesAnke NemirovskyPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Reten Modern Dressing 2023 PKDMTDocument51 pagesReten Modern Dressing 2023 PKDMTMasros TukiranPas encore d'évaluation
- End of Shift Competency ChecklistDocument3 pagesEnd of Shift Competency ChecklistRnskillsPas encore d'évaluation
- Icu GuidebookDocument43 pagesIcu Guidebookdrimran570100% (5)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- NCP Post DebridementDocument7 pagesNCP Post Debridementtintinlovessu100% (2)
- Anorectal Conditions: Manisha Thapa Roll No: 06 BSN 2 YearDocument11 pagesAnorectal Conditions: Manisha Thapa Roll No: 06 BSN 2 YearManjesh Mishra XettriPas encore d'évaluation
- Write Up TBDocument8 pagesWrite Up TBARGIEPas encore d'évaluation
- The American Academy of PediatricsDocument2 pagesThe American Academy of PediatricsrahmanugrohoPas encore d'évaluation
- 7 Doh Approved Herbal Medicine: Pictures Indicataion Contraindication Nursing ResponsibilityDocument5 pages7 Doh Approved Herbal Medicine: Pictures Indicataion Contraindication Nursing ResponsibilityShaira Ann CalambaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Thyroid Disease in PregnancyDocument36 pagesThyroid Disease in Pregnancypeni_dwiPas encore d'évaluation
- Wegener's GranulomatosisDocument43 pagesWegener's GranulomatosisOlga GoryachevaPas encore d'évaluation
- CMO No 25 Series 2021 PSG For BS PharmacyDocument49 pagesCMO No 25 Series 2021 PSG For BS PharmacyIrenelle OdtojanPas encore d'évaluation
- Child Health Nursin11.Doc123Document400 pagesChild Health Nursin11.Doc123Destaalem GhinPas encore d'évaluation
- Summary For The Case Study On MastectomyDocument2 pagesSummary For The Case Study On MastectomyNishi SharmaPas encore d'évaluation
- The Newcastle Upon Tyne Hospitals NHS Foundation Trust Asepsis PolicyDocument10 pagesThe Newcastle Upon Tyne Hospitals NHS Foundation Trust Asepsis Policyyousrazeidan1979Pas encore d'évaluation
- Fitness & Wellness Industry in IndiaDocument12 pagesFitness & Wellness Industry in IndiaPrince SinghPas encore d'évaluation
- StammBerger 1990Document14 pagesStammBerger 1990OtorrinolaringologíaLoayza100% (1)
- Basics Concept of Pharmacoepidemiology: Yusi AnggrianiDocument21 pagesBasics Concept of Pharmacoepidemiology: Yusi AnggrianiDjuffiNelwanPas encore d'évaluation
- Airway Management For Oral and Maxillofacial SurgeryDocument9 pagesAirway Management For Oral and Maxillofacial SurgerykrazeedoctorPas encore d'évaluation
- Health Promotion in Nursing 3rd Edition Maville Test BankDocument5 pagesHealth Promotion in Nursing 3rd Edition Maville Test Bankrichardfranklinsanyzqokdg100% (15)
- Closed Comminutive Fracture Middle Left Clavicle Allman Classification Group IDocument32 pagesClosed Comminutive Fracture Middle Left Clavicle Allman Classification Group IWilliamtatokieesz Tembokrumahampebenjol-benjolPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)