Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Easier Shorter Safer BirthDocument53 pagesEasier Shorter Safer Birthmw101mw100% (1)
- Maxillofacial TraumaDocument70 pagesMaxillofacial Traumaeman_879_123456Pas encore d'évaluation
- Ventilator Care 1Document11 pagesVentilator Care 1Friends ForeverPas encore d'évaluation
- MR Angiography: Divya NinanDocument52 pagesMR Angiography: Divya NinanBenjamin Barsouma Mathew100% (1)
- AOMSI MC2022 ScheduleDocument10 pagesAOMSI MC2022 ScheduleDarain ShahidPas encore d'évaluation
- Lower Limb Question Bank by Vincent Chidiebube Orji-1Document4 pagesLower Limb Question Bank by Vincent Chidiebube Orji-1Mumu MumuPas encore d'évaluation
- DR Jay CalvertDocument2 pagesDR Jay CalvertJay Calvert100% (6)
- CPG-Coronary Artery Disease (2014)Document120 pagesCPG-Coronary Artery Disease (2014)lovelots1234Pas encore d'évaluation
- DH 220 - Specialty Office Visit - Teagan RubidaDocument7 pagesDH 220 - Specialty Office Visit - Teagan Rubidaapi-725916152Pas encore d'évaluation
- Name: Rikki Mae P. Bueno Section: BSN-1105Document1 pageName: Rikki Mae P. Bueno Section: BSN-1105Rikki Mae BuenoPas encore d'évaluation
- Maxillofacial Reconstruction 2013Document237 pagesMaxillofacial Reconstruction 2013Mohammed Qasim Al-WataryPas encore d'évaluation
- 2020 DNB AnesthesiaDocument33 pages2020 DNB AnesthesiasreesaichowdaryPas encore d'évaluation
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosPas encore d'évaluation
- Teknik Operasi Pericardial Window LiusDocument23 pagesTeknik Operasi Pericardial Window LiusDeddy Guu100% (1)
- 4.29a - The Lower Extremities - Gluteal Region, Anterolateral ThighDocument14 pages4.29a - The Lower Extremities - Gluteal Region, Anterolateral ThighShariq ArshadPas encore d'évaluation
- Wound Dehiscence Over RegenerateDocument26 pagesWound Dehiscence Over RegenerateasioquaPas encore d'évaluation
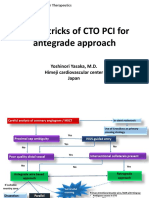
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocument21 pagesTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazurePas encore d'évaluation
- Skill 20 Bag Valve Mask (BVM) VentilationDocument2 pagesSkill 20 Bag Valve Mask (BVM) VentilationThulasi tootsiePas encore d'évaluation
- ASSSSDocument21 pagesASSSSACERET, IVAN LAURENTINE G.Pas encore d'évaluation
- MCQDocument4 pagesMCQleonPas encore d'évaluation
- Philips InnerCool Product BrochureDocument8 pagesPhilips InnerCool Product BrochurephilipsinnercoolPas encore d'évaluation
- The Swing Lock Denture Its Use in Conventional Removable Partial Denture Prosthodontics PDFDocument3 pagesThe Swing Lock Denture Its Use in Conventional Removable Partial Denture Prosthodontics PDFscott_c_kane100% (1)
- Daftar Pustaka Frozen ShoulderDocument3 pagesDaftar Pustaka Frozen ShoulderMuhammad Faza NaufalPas encore d'évaluation
- Timing of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyDocument3 pagesTiming of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyJuan J. Acosta VelásquezPas encore d'évaluation
- Cataract Surgery Side EffectsDocument4 pagesCataract Surgery Side EffectsEye spacialistPas encore d'évaluation
- 9 9 2023Document10 pages9 9 2023hoangnam147680Pas encore d'évaluation
- Stroke EssentialsDocument44 pagesStroke Essentialsapi-452244667Pas encore d'évaluation
- Reasons For TonsillectomyDocument8 pagesReasons For TonsillectomyRasdumi100% (1)
- Inguinal Hernia EpidemiologyDocument5 pagesInguinal Hernia Epidemiologymelon segerPas encore d'évaluation
- Incise Drape CatalogueDocument10 pagesIncise Drape CatalogueShadreck MabvoroPas encore d'évaluation