Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Literature 3 PDFDocument1 pageLiterature 3 PDFVhiena ShittaPas encore d'évaluation
- Literature 3Document1 pageLiterature 3Vhiena ShittaPas encore d'évaluation
- Alternative Therapies in Health and Medicine Jan 2000 6, 1 ProquestDocument8 pagesAlternative Therapies in Health and Medicine Jan 2000 6, 1 ProquestVhiena ShittaPas encore d'évaluation
- Learning Zone: An Overview of Cardiovascular Disease Risk AssessmentDocument10 pagesLearning Zone: An Overview of Cardiovascular Disease Risk AssessmentVhiena ShittaPas encore d'évaluation
- Hipersensitivitas 3Document9 pagesHipersensitivitas 3Vhiena ShittaPas encore d'évaluation
- Nurse Practitioner Sep 2000 25, 9 ProquestDocument8 pagesNurse Practitioner Sep 2000 25, 9 ProquestVhiena ShittaPas encore d'évaluation
- 0301wheel ManualDocument366 pages0301wheel ManualVhiena ShittaPas encore d'évaluation
- Incidental Diagnosis of Intradural Lumbar Disc Herniation During Discography: A Case ReportDocument6 pagesIncidental Diagnosis of Intradural Lumbar Disc Herniation During Discography: A Case ReportVhiena ShittaPas encore d'évaluation
- Multiple Sclerosis and Mobility-Related Assistive Technology: Systematic Review of LiteratureDocument12 pagesMultiple Sclerosis and Mobility-Related Assistive Technology: Systematic Review of LiteratureVhiena ShittaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Grandjean 2000Document13 pagesGrandjean 2000Ivan VeriswanPas encore d'évaluation
- HenryDocument21 pagesHenryEvans rizqanPas encore d'évaluation
- Manajemen NyeriDocument8 pagesManajemen Nyeriagung yulisaputraPas encore d'évaluation
- Asia Pacific Occupational Therapy Congress ProgrammeDocument8 pagesAsia Pacific Occupational Therapy Congress ProgrammeRLedgerdPas encore d'évaluation
- Computational BioengineeringDocument480 pagesComputational Bioengineeringscribd990Pas encore d'évaluation
- Pathology 2 TND LiveDocument38 pagesPathology 2 TND Livepavan kumarPas encore d'évaluation
- 04IJPHY907Document8 pages04IJPHY907ize browniezPas encore d'évaluation
- AAA Mixed Pain SMGDocument37 pagesAAA Mixed Pain SMGandhita96Pas encore d'évaluation
- Skan Respiro PlusDocument3 pagesSkan Respiro PlusAparajitaSaha100% (1)
- Para Instwise Adm Af Reporting Cancel r1Document639 pagesPara Instwise Adm Af Reporting Cancel r1Rutvik DhoriyaPas encore d'évaluation
- The Influence of Fine Excipient Particles On The Performance PDFDocument10 pagesThe Influence of Fine Excipient Particles On The Performance PDFahmedsidalaPas encore d'évaluation
- Clinical Pharmacology in Healthcare, Teaching and ResearchDocument80 pagesClinical Pharmacology in Healthcare, Teaching and ResearchVNcomer100% (1)
- The House Tree and Person TestDocument10 pagesThe House Tree and Person TestRidaPas encore d'évaluation
- Sex Love and Mental IllnessDocument160 pagesSex Love and Mental IllnessCristina Vișan100% (3)
- Garv ResumeDocument5 pagesGarv Resumegarv_pt100% (1)
- 2016 PSSI-5 PsychologicalAssessmentDocument8 pages2016 PSSI-5 PsychologicalAssessmentLitzaPas encore d'évaluation
- Happiful June 2022Document92 pagesHappiful June 2022Лера СавченкоPas encore d'évaluation
- Advancedcancer PDFDocument64 pagesAdvancedcancer PDFAnonymous YdFUaW6fBPas encore d'évaluation
- Nutrition and Fitness by Marshall Cavendish PDFDocument209 pagesNutrition and Fitness by Marshall Cavendish PDFWinioliski Rohi BirePas encore d'évaluation
- Malignant 2021 480p WEB-DL x264 400MB-Pahe inDocument59 pagesMalignant 2021 480p WEB-DL x264 400MB-Pahe inBranislav IvanovicPas encore d'évaluation
- SyncopeDocument105 pagesSyncopeJohn DasPas encore d'évaluation
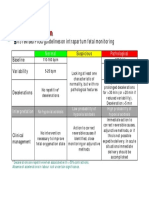
- CTG Classification PDFDocument1 pageCTG Classification PDFganotPas encore d'évaluation
- ReserarchDocument4 pagesReserarchapi-287181456Pas encore d'évaluation
- 12 Potent Acupressure Points To Cure VertigoDocument14 pages12 Potent Acupressure Points To Cure VertigoChetna Kanchan BhagatPas encore d'évaluation
- Frozen ShoulderDocument44 pagesFrozen ShoulderEspers BluesPas encore d'évaluation
- SYLLABUSDocument5 pagesSYLLABUSArc Angelus Civitas School100% (1)
- Child Art Therapy (PDFDrive)Document467 pagesChild Art Therapy (PDFDrive)Ilsu Pamuk100% (5)
- Askep OsteomielitisDocument12 pagesAskep OsteomielitisSeny triastutikPas encore d'évaluation
- FC Paed (SA) Part II Past Papers - 2011 Sept 8-4-2014Document5 pagesFC Paed (SA) Part II Past Papers - 2011 Sept 8-4-2014matentenPas encore d'évaluation
- Halterman Technique For The Treatment of Ectopically Erupting Permanent First MolarsDocument7 pagesHalterman Technique For The Treatment of Ectopically Erupting Permanent First MolarsIOSRjournalPas encore d'évaluation