Vous aimerez peut-être aussi
- Emergency Postcoital ContraceptionDocument4 pagesEmergency Postcoital ContraceptionCostin VrabiePas encore d'évaluation
- Practice Bullet In: Emergency ContraceptionDocument11 pagesPractice Bullet In: Emergency ContraceptionYosep SutandarPas encore d'évaluation
- Emergency Contraception 2015Document11 pagesEmergency Contraception 2015ErickPas encore d'évaluation
- Recent Advances in ContraceptionDocument12 pagesRecent Advances in ContraceptionSandhya sPas encore d'évaluation
- Ulipristal Acetate For Emergency ContraceptionDocument8 pagesUlipristal Acetate For Emergency ContraceptionAnonymous SDUIPeqXPas encore d'évaluation
- Anticincepcion de EmergenciaDocument10 pagesAnticincepcion de EmergenciaDebbie GuerreroPas encore d'évaluation
- Emergency ContraceptionDocument6 pagesEmergency ContraceptionAHm'd MetwallyPas encore d'évaluation
- Emergency ContraceptionDocument6 pagesEmergency ContraceptionAHm'd MetwallyPas encore d'évaluation
- Shrader2011 Updates in Hormonal Emergency ContraceptionDocument9 pagesShrader2011 Updates in Hormonal Emergency ContraceptionAdityaWijayaPas encore d'évaluation
- Ulipristal Acetate: Review of Its Use in Emergency ContraseptionDocument12 pagesUlipristal Acetate: Review of Its Use in Emergency ContraseptionAnonymous SDUIPeqXPas encore d'évaluation
- Emergency ContraceptionDocument7 pagesEmergency Contraceptionyogita_itsme7560Pas encore d'évaluation
- Delivers 0.120 mg/0.015 MG Per DayDocument6 pagesDelivers 0.120 mg/0.015 MG Per DayscrewthisPas encore d'évaluation
- Emergency ContraceptionDocument11 pagesEmergency ContraceptionindeenikePas encore d'évaluation
- Refernsi KontraDocument19 pagesRefernsi Kontraekaseptiani312Pas encore d'évaluation
- Copper Intrauterine DeviceDocument2 pagesCopper Intrauterine DeviceajenkajenkPas encore d'évaluation
- Ulipristal Acetate - A New Emergency ContraceptiveDocument4 pagesUlipristal Acetate - A New Emergency ContraceptiveAnonymous SDUIPeqXPas encore d'évaluation
- Practice Bulletin: Long-Acting Reversible Contraception: Implants and Intrauterine DevicesDocument13 pagesPractice Bulletin: Long-Acting Reversible Contraception: Implants and Intrauterine Devicesputri azzahraPas encore d'évaluation
- Family Planning and ContraceptionDocument39 pagesFamily Planning and ContraceptionDitaleniPas encore d'évaluation
- Emergency Contraception: "The Morning-After Pill"Document24 pagesEmergency Contraception: "The Morning-After Pill"Dr. Sujnanendra MishraPas encore d'évaluation
- GNIPST Bulletin 21.4Document17 pagesGNIPST Bulletin 21.4Gnipst BulletinPas encore d'évaluation
- Evidace Based ECDocument15 pagesEvidace Based ECRana Yuda StiraPas encore d'évaluation
- Combined Hormonal Contraception: What's New ?Document5 pagesCombined Hormonal Contraception: What's New ?sivaPas encore d'évaluation
- Obs Gyn שחזוריםDocument44 pagesObs Gyn שחזוריםLaith Bajis NassarPas encore d'évaluation
- Depo-Provera - Wikipedia, The Free EncyclopediaDocument13 pagesDepo-Provera - Wikipedia, The Free EncyclopediaKhateeb Ul Islam QadriPas encore d'évaluation
- Progestin Only ContraceptionDocument4 pagesProgestin Only ContraceptionTareq SawanPas encore d'évaluation
- 2006 Understanding Emergency ContraceptionDocument4 pages2006 Understanding Emergency ContraceptiontaikucinglohPas encore d'évaluation
- Pharmacology Reproductive Maternity NewbornDocument24 pagesPharmacology Reproductive Maternity Newbornamasoud96 amasoud96Pas encore d'évaluation
- CONTRACEPTION TeachingDocument46 pagesCONTRACEPTION TeachingsaufisafingiPas encore d'évaluation
- Peace Corps MTG FOIA General Medicine 2Document191 pagesPeace Corps MTG FOIA General Medicine 2Accessible Journal Media: Peace Corps DocumentsPas encore d'évaluation
- Contraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToDocument22 pagesContraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToAmmarPas encore d'évaluation
- Intra Uterine Device: Ruswana Anwar, DR, Spog (K), MkesDocument69 pagesIntra Uterine Device: Ruswana Anwar, DR, Spog (K), MkesMochammad Rizal AttamimiPas encore d'évaluation
- EnglishDocument4 pagesEnglishAhmed AbdulsaborPas encore d'évaluation
- Administration of Hormonal Contraceptive Drugs: A Quick Reference Guide For CliniciansDocument28 pagesAdministration of Hormonal Contraceptive Drugs: A Quick Reference Guide For Clinicianshesham00100Pas encore d'évaluation
- Contraceptionmethods 150710090424 Lva1 App6891 PDFDocument56 pagesContraceptionmethods 150710090424 Lva1 App6891 PDFeffiniasiregarPas encore d'évaluation
- ProQuestDocuments 2023 01 11Document4 pagesProQuestDocuments 2023 01 11restu pangestutiPas encore d'évaluation
- Hormonal Emergency Contraception G16 v5Document11 pagesHormonal Emergency Contraception G16 v5Paolo MaurelliPas encore d'évaluation
- Contraception: Heidery - Class DR. Hanaa Al 5 GynaecologyDocument11 pagesContraception: Heidery - Class DR. Hanaa Al 5 Gynaecologyzianab aliPas encore d'évaluation
- Contraception & HRTDocument14 pagesContraception & HRTWheezy BruhPas encore d'évaluation
- Intrauterine Contraception: ReviewDocument9 pagesIntrauterine Contraception: ReviewSaeed HasanPas encore d'évaluation
- Family Planning and AbortionDocument85 pagesFamily Planning and AbortionSheena PasionPas encore d'évaluation
- Gynecology - ContraceptionDocument10 pagesGynecology - ContraceptionparaschoumariaPas encore d'évaluation
- ContraceptionDocument17 pagesContraceptionMohan bhargavPas encore d'évaluation
- Ceftriaxone, Misoprostol, OxytocinDocument4 pagesCeftriaxone, Misoprostol, OxytocinKrizia Bonilla100% (1)
- Emergency Contraception: Clinical PracticeDocument7 pagesEmergency Contraception: Clinical Practicedectria puspithoPas encore d'évaluation
- ContraceptivesDocument8 pagesContraceptivesRadowan AhmadPas encore d'évaluation
- Aromatase Inhibitors For Ovulation Induction and Ovarian StimulationDocument13 pagesAromatase Inhibitors For Ovulation Induction and Ovarian StimulationGinecologia Aseptică 1Pas encore d'évaluation
- Lec 13. ContraceptivesDocument41 pagesLec 13. Contraceptivesshahnaz AyasrahPas encore d'évaluation
- ContraceptionDocument38 pagesContraceptionMalk OmryPas encore d'évaluation
- Emergency ContraceptionDocument14 pagesEmergency ContraceptionJEFFERSON MUÑOZPas encore d'évaluation
- Current Controversies With Oral Emergency Contraception: A ReviewDocument19 pagesCurrent Controversies With Oral Emergency Contraception: A ReviewNEHEMIAS PAYARESPas encore d'évaluation
- Hysteroscopic Sterilization ESSUREDocument13 pagesHysteroscopic Sterilization ESSUREXimena OrtegaPas encore d'évaluation
- Insertion and Removal of Intrauterine Devices-AAFPDocument8 pagesInsertion and Removal of Intrauterine Devices-AAFPnouval_iqbalPas encore d'évaluation
- Emergency ContraceptionDocument20 pagesEmergency Contraceptionnityaprasanta4679100% (1)
- Indocollyre PDFDocument6 pagesIndocollyre PDFUpik MoritaPas encore d'évaluation
- The Long Acting Reversible Contraceptive (LARC) GuidelineDocument20 pagesThe Long Acting Reversible Contraceptive (LARC) GuidelineYinlerLeePas encore d'évaluation
- A Guia Uso Implantes Progestgenos PDFDocument32 pagesA Guia Uso Implantes Progestgenos PDFAnaMariaVilcaMuñozPas encore d'évaluation
- Miso Fact Sheet ENG-2016Document4 pagesMiso Fact Sheet ENG-2016Hoplar DoreenPas encore d'évaluation
- Fertility Control: (Contraception)Document68 pagesFertility Control: (Contraception)SaraMohammedPas encore d'évaluation
- Chemical Abortion 7-21Document5 pagesChemical Abortion 7-21sanshinroxPas encore d'évaluation
- My Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsD'EverandMy Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsPas encore d'évaluation
- CR 3-23 A-FGJ-A-E-HQQE: Position Qty. Description Single PriceDocument7 pagesCR 3-23 A-FGJ-A-E-HQQE: Position Qty. Description Single PriceIshak AnsarPas encore d'évaluation
- Hund T FindingsDocument4 pagesHund T FindingsIshak AnsarPas encore d'évaluation
- Cover Sheet: Print Form Clear FormDocument1 pageCover Sheet: Print Form Clear FormIshak AnsarPas encore d'évaluation
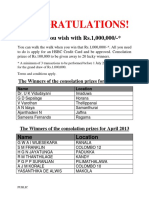
- Congratulations!: Live As You Wish With Rs.1,000,000Document1 pageCongratulations!: Live As You Wish With Rs.1,000,000Ishak AnsarPas encore d'évaluation
- Department of Electronic Engineering: Final Year Project ReportDocument59 pagesDepartment of Electronic Engineering: Final Year Project ReportIshak AnsarPas encore d'évaluation
- Calendar 2012 BlackDocument1 pageCalendar 2012 BlackIshak AnsarPas encore d'évaluation
- C02-Fundamentals of Financial Accounting: Sample Exam PaperDocument15 pagesC02-Fundamentals of Financial Accounting: Sample Exam PaperIshak AnsarPas encore d'évaluation
- Central Bank of Sri Lanka: Premier Financial InstitutionDocument1 pageCentral Bank of Sri Lanka: Premier Financial InstitutionIshak AnsarPas encore d'évaluation
- Project Titles and Supervisors-2011Document24 pagesProject Titles and Supervisors-2011Ishak AnsarPas encore d'évaluation
- RE and Dfhgrapid ProductDocument6 pagesRE and Dfhgrapid ProductIshak AnsarPas encore d'évaluation
- Semi Log Graph Paper BWDocument1 pageSemi Log Graph Paper BWIshak AnsarPas encore d'évaluation
- Motor BookDocument252 pagesMotor BookKyaw KhPas encore d'évaluation
- Dr. N. Kumarappan IE (I) Council Candidate - Electrical DivisionDocument1 pageDr. N. Kumarappan IE (I) Council Candidate - Electrical Divisionshanmugasundaram32Pas encore d'évaluation
- Potassium Permanganate CARUSOL CarusCoDocument9 pagesPotassium Permanganate CARUSOL CarusColiebofreakPas encore d'évaluation
- Masters Thesis Benyam 2011Document156 pagesMasters Thesis Benyam 2011TechBoy65Pas encore d'évaluation
- Cisco Nexus 7000 Introduction To NX-OS Lab GuideDocument38 pagesCisco Nexus 7000 Introduction To NX-OS Lab Guiderazzzzzzzzzzz100% (1)
- Two Occult Philosophers in The Elizabethan Age: by Peter ForshawDocument10 pagesTwo Occult Philosophers in The Elizabethan Age: by Peter ForshawFrancesco VinciguerraPas encore d'évaluation
- Finite Element Modeling Analysis of Nano Composite Airfoil StructureDocument11 pagesFinite Element Modeling Analysis of Nano Composite Airfoil StructureSuraj GautamPas encore d'évaluation
- Rotex GS Zero-Backlash Shaft CouplingDocument19 pagesRotex GS Zero-Backlash Shaft CouplingIrina DimitrovaPas encore d'évaluation
- Recruitment Process Outsourcing PDFDocument4 pagesRecruitment Process Outsourcing PDFDevesh NamdeoPas encore d'évaluation
- 04 DosimetryDocument104 pages04 DosimetryEdmond ChiangPas encore d'évaluation
- Jo - Mc.Donough. ESP in Perspective A Practical Guide. London. Collin ELT. 1984. p.3Document6 pagesJo - Mc.Donough. ESP in Perspective A Practical Guide. London. Collin ELT. 1984. p.3Falihatul Kholidiyah100% (1)
- NUR 104 Nursing Process MY NOTESDocument77 pagesNUR 104 Nursing Process MY NOTESmeanne073100% (1)
- Application of SPACE MatrixDocument11 pagesApplication of SPACE Matrixdecker444975% (4)
- Self Regulated StudyDocument6 pagesSelf Regulated StudyAdelheyde HelenePas encore d'évaluation
- Pediatric Infectious DiseasesDocument3 pagesPediatric Infectious DiseasesAiri FirdausiaPas encore d'évaluation
- Procedure For Non Hazardous Waste ManagementDocument6 pagesProcedure For Non Hazardous Waste ManagementPaddyPas encore d'évaluation
- Happiest Refugee Coursework 2013Document10 pagesHappiest Refugee Coursework 2013malcrowe100% (2)
- Primefaces Users Guide 3 5cDocument497 pagesPrimefaces Users Guide 3 5calvarolucasPas encore d'évaluation
- VRF-SLB013-EN - 0805115 - Catalogo Ingles 2015 PDFDocument50 pagesVRF-SLB013-EN - 0805115 - Catalogo Ingles 2015 PDFJhon Lewis PinoPas encore d'évaluation
- EUROJAM Diary3Document4 pagesEUROJAM Diary3Susan BakerPas encore d'évaluation
- Zara Case StudyDocument26 pagesZara Case StudySeminarskiRadovi100% (2)
- Iso 27001 Requirementsandnetwrixfunctionalitymapping 1705578827995Document33 pagesIso 27001 Requirementsandnetwrixfunctionalitymapping 1705578827995Tassnim Ben youssefPas encore d'évaluation
- Ofsaai Ic 72 E22351 01Document312 pagesOfsaai Ic 72 E22351 01Mohamed AbrarPas encore d'évaluation
- DbmsDocument5 pagesDbmsRohit KushwahaPas encore d'évaluation
- Important Points in SurveyingDocument4 pagesImportant Points in SurveyingAnand BossPas encore d'évaluation
- ArticleDocument9 pagesArticleElly SufriadiPas encore d'évaluation
- Device InfoDocument3 pagesDevice InfoGrig TeoPas encore d'évaluation
- თინათინ ზურაბიშვილი, თვისებრივი მეთოდებიDocument111 pagesთინათინ ზურაბიშვილი, თვისებრივი მეთოდებიNino LomaiaPas encore d'évaluation
- Digital Control Engineering 2nd Edition Fadali Solutions Manual PDFDocument3 pagesDigital Control Engineering 2nd Edition Fadali Solutions Manual PDFMohammed SalahPas encore d'évaluation
- STORIESDocument18 pagesSTORIESHaRa TPas encore d'évaluation