Vous aimerez peut-être aussi
- Endocrinology Notes for Medical StudentsD'EverandEndocrinology Notes for Medical StudentsÉvaluation : 4 sur 5 étoiles4/5 (1)
- Musculoskeletal PharmacologyDocument18 pagesMusculoskeletal PharmacologyBLEEMAGE100% (2)
- Top 300 Drugs Pocket Reference Guide (2021 Edition)D'EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Évaluation : 5 sur 5 étoiles5/5 (1)
- Pharm MnemonicsDocument33 pagesPharm MnemonicsThomson George75% (4)
- Pharma MnemonicsDocument12 pagesPharma MnemonicsUsman Ali Akbar100% (1)
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDocument18 pagesPharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- Drugs MnemonicsDocument6 pagesDrugs MnemonicsDarrylJavier100% (1)
- Pharmacology MnemonicsDocument17 pagesPharmacology MnemonicsJuvenis SampangPas encore d'évaluation
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1D'EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1Évaluation : 5 sur 5 étoiles5/5 (2)
- Drug ChartDocument8 pagesDrug Chartstudentalwaysstudy100% (1)
- ANS DrugsDocument2 pagesANS Drugsmed testPas encore d'évaluation
- Ninja - Anti-HTN PDFDocument6 pagesNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Drug Mechanism Clincal Use Side Effects Antifungal: Amphote Ricin BDocument30 pagesDrug Mechanism Clincal Use Side Effects Antifungal: Amphote Ricin BCess Lagera Ybanez0% (1)
- Pharmacy MnenomicsDocument12 pagesPharmacy MnenomicsNaresh BabuPas encore d'évaluation
- Ninja - Anemias PDFDocument1 pageNinja - Anemias PDFErica Hyeyeon LeePas encore d'évaluation
- Pharmacology MnemonicsDocument19 pagesPharmacology MnemonicsAl-nazer Azer Al100% (5)
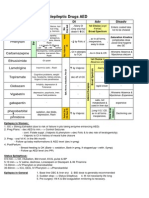
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Pas encore d'évaluation
- Drug SuffixesDocument3 pagesDrug SuffixesjeromeasuncionPas encore d'évaluation
- Pharmacology Complete Drug TableDocument6 pagesPharmacology Complete Drug Tableninja-2001100% (4)
- Pharmacology Chart 3Document2 pagesPharmacology Chart 3Omar ClorPas encore d'évaluation
- Mnemonics For PharmacologyDocument14 pagesMnemonics For Pharmacologyloftysingh100% (8)
- Pharmacology ChartDocument6 pagesPharmacology ChartPaula67% (3)
- Pharmacology MnemonicsDocument24 pagesPharmacology MnemonicsMrs3carpediem0% (1)
- Review Handouts For Medical Pharmacology PDFDocument21 pagesReview Handouts For Medical Pharmacology PDFAndres F. TorresPas encore d'évaluation
- Ninja - Cholinergic Drugs PDFDocument4 pagesNinja - Cholinergic Drugs PDFErica Hyeyeon Lee100% (2)
- Muscarine & Nicotinic: ReceptorDocument26 pagesMuscarine & Nicotinic: ReceptorCess Lagera Ybanez88% (16)
- Pharmacology ChartDocument23 pagesPharmacology ChartKelly Milaski0% (1)
- Patho Physiology Bible: Over 70 Concept MapsDocument139 pagesPatho Physiology Bible: Over 70 Concept Mapslauramphs79100% (5)
- Antibiotics ChartDocument10 pagesAntibiotics Chartadom09Pas encore d'évaluation
- Pharmacology Important Things To RememberDocument5 pagesPharmacology Important Things To RememberHydie100% (1)
- Pharmacology Mnemonics (Part 01) by M IhtishamDocument32 pagesPharmacology Mnemonics (Part 01) by M Ihtishammuhammad ihtisham ul hassan100% (1)
- Opioids PDFDocument2 pagesOpioids PDFErica Hyeyeon LeePas encore d'évaluation
- Antibiotics Cheat SheetDocument2 pagesAntibiotics Cheat SheetAlejandro Rodas Salinas100% (1)
- Pharmacology - Drug ChartsDocument39 pagesPharmacology - Drug ChartsAsim Ishaq100% (5)
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDocument16 pagesThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- Ninja - Antiarrhythmic Drugs PDFDocument7 pagesNinja - Antiarrhythmic Drugs PDFErica Hyeyeon Lee100% (1)
- MBBS Pharmacology PDFDocument20 pagesMBBS Pharmacology PDFAdeeb Aiman Rosli100% (6)
- Common Drugs ChartDocument15 pagesCommon Drugs Chartforminsko100% (1)
- Inhibit Clasification Antibiotics: (Broad Spectrum) (Narrow Spectrum)Document1 pageInhibit Clasification Antibiotics: (Broad Spectrum) (Narrow Spectrum)SY WongPas encore d'évaluation
- Pharmacology Cheat Sheet - Generic Drug Stems - NurseslabsDocument12 pagesPharmacology Cheat Sheet - Generic Drug Stems - NurseslabsKc Mea Paran BorjaPas encore d'évaluation
- Antibiotics Chart 2Document10 pagesAntibiotics Chart 2Vee MendPas encore d'évaluation
- Major Pharm ReviewDocument14 pagesMajor Pharm Reviewsarahpierre10100% (3)
- Pharm Drug ListDocument17 pagesPharm Drug Listanon_523534678Pas encore d'évaluation
- Pharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, NifedipineDocument7 pagesPharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, Nifedipinecherrybombaz100% (4)
- Penicillins Pen&G Pen&V: T.%pallidum% (Syphilis)Document1 pagePenicillins Pen&G Pen&V: T.%pallidum% (Syphilis)gregoryvo100% (5)
- Pharmacology Mnemonics.Document16 pagesPharmacology Mnemonics.Shan Shani67% (3)
- Drug of ChoiceDocument2 pagesDrug of ChoiceRia Tiglao Fortugaliza100% (1)
- CardionotesDocument5 pagesCardionotesNichole Coletta100% (1)
- Osmosis Acute Coronary SyndromesDocument5 pagesOsmosis Acute Coronary Syndromesvalentinabil3Pas encore d'évaluation
- Sphere: These DiarrheaDocument3 pagesSphere: These Diarrheamed testPas encore d'évaluation
- Respiratory Tract PharmacologyDocument68 pagesRespiratory Tract PharmacologyRohaan SharmaPas encore d'évaluation
- Antiadrenergic DrugsDocument44 pagesAntiadrenergic DrugsHUZAIFA YAMAANPas encore d'évaluation
- Pcol MnemonicsDocument12 pagesPcol MnemonicsJustine Rubillete Mendoza MarianoPas encore d'évaluation
- Drug StudyDocument6 pagesDrug StudyBij Hilario100% (1)
- Tufts Med ListDocument5 pagesTufts Med ListMarisa Deana Pontrelli100% (1)
- Communicable Disease Nursing Clinical FocusDocument2 pagesCommunicable Disease Nursing Clinical Focusrceponelas1127Pas encore d'évaluation
- Typical Signs and Symptoms of Mental Illness 1Document3 pagesTypical Signs and Symptoms of Mental Illness 1Sunny MaePas encore d'évaluation
- Telehealth PaperDocument19 pagesTelehealth PaperLalitha PerumalPas encore d'évaluation
- Psyche ReviewerDocument13 pagesPsyche ReviewerKem100% (1)
- Vyvanse CouponDocument6 pagesVyvanse CouponAnna PottsPas encore d'évaluation
- Medical Transcription - Operative ReportDocument2 pagesMedical Transcription - Operative Reportmyahuynh25100% (1)
- One Compartment Open ModelDocument81 pagesOne Compartment Open Modelanon_937994778Pas encore d'évaluation
- Retinopathy of PrematurityDocument15 pagesRetinopathy of Prematuritymarissa ulkhairPas encore d'évaluation
- DysmenorrheaDocument28 pagesDysmenorrheaDr Munira MalikPas encore d'évaluation
- Oral Manifestations of Connective Tissue Disease (CTDDocument34 pagesOral Manifestations of Connective Tissue Disease (CTDFatin Nabihah Jamil67% (3)
- Top 100 DrugsDocument5 pagesTop 100 DrugsGiacenPas encore d'évaluation
- Pysch Nursing ReviewerDocument72 pagesPysch Nursing ReviewerKristeen Camille ValentinoPas encore d'évaluation
- DOH AO 2016-0041 Prevention and Management of Abortion ComplicationsDocument13 pagesDOH AO 2016-0041 Prevention and Management of Abortion ComplicationsGa B B Orlongan100% (1)
- Easa Use of Medication in The Aviation EnvironmentDocument8 pagesEasa Use of Medication in The Aviation Environmentfox_llnvjv373Pas encore d'évaluation
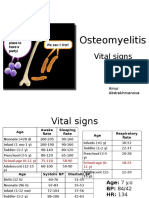
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaPas encore d'évaluation
- Comprehension Book Grade 12Document66 pagesComprehension Book Grade 12milkovicius0% (3)
- Patient Centered in Heart Failure PatientsDocument10 pagesPatient Centered in Heart Failure PatientsberylianamayaPas encore d'évaluation
- Gluten-Casein Peptides TestDocument2 pagesGluten-Casein Peptides TestjmkcbePas encore d'évaluation
- Intrapartum NCM 107Document8 pagesIntrapartum NCM 107Kimberly Sharah Mae FortunoPas encore d'évaluation
- Inference Based Therapy Fo BDD PDFDocument10 pagesInference Based Therapy Fo BDD PDFGeniefe VivendaPas encore d'évaluation
- Hospital Review 2017Document32 pagesHospital Review 2017NM Atif100% (5)
- Padma Bhushan Ashtavaidyan E T Narayanan MoossDocument1 pagePadma Bhushan Ashtavaidyan E T Narayanan MoossK Govindan NampoothiryPas encore d'évaluation
- Perforative PeritonitisDocument58 pagesPerforative PeritonitisSangeeta BSR82% (17)
- KELOMPOK 1 - RS2 - PRAKTIK BAHASA INGGRIS DetailDocument12 pagesKELOMPOK 1 - RS2 - PRAKTIK BAHASA INGGRIS Detailseren agathaPas encore d'évaluation
- Woodcutters TechniqueDocument3 pagesWoodcutters TechniqueToo SmallPas encore d'évaluation
- Paper 5 Review The Literature of Balanced Scorecard and Performance Measurement 1Document15 pagesPaper 5 Review The Literature of Balanced Scorecard and Performance Measurement 1Kepher OnukoPas encore d'évaluation
- Performance Improvement Plan Template 1 - 908445459Document3 pagesPerformance Improvement Plan Template 1 - 908445459api-534828007Pas encore d'évaluation
- PGHHHMDocument30 pagesPGHHHMDaipayan Lodh75% (4)
- Introduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologyDocument26 pagesIntroduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologymochkurniawanPas encore d'évaluation
- Eye Path12Document45 pagesEye Path12JillKellyPas encore d'évaluation