Vous aimerez peut-être aussi
- 68 ClassificationDocument8 pages68 ClassificationClaudix PuccaPas encore d'évaluation
- Brainstem Glioma in AdultsDocument57 pagesBrainstem Glioma in AdultsescherianPas encore d'évaluation
- A-Z Health Guide From Webmd: Medical Tests: Computed Tomography (CT) Scan of The Body Test OverviewDocument16 pagesA-Z Health Guide From Webmd: Medical Tests: Computed Tomography (CT) Scan of The Body Test Overviewc4rm3LPas encore d'évaluation
- Klasifikasi Tumor OtakDocument81 pagesKlasifikasi Tumor Otaknovy rosalia chandraPas encore d'évaluation
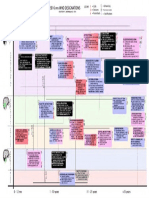
- CNS Tumor MapDocument1 pageCNS Tumor MapaquavindPas encore d'évaluation
- EASL Haemochromatosis GuidelinesDocument26 pagesEASL Haemochromatosis Guidelinesmonday125Pas encore d'évaluation
- Modern Alegria Resume by SlidesgoDocument32 pagesModern Alegria Resume by SlidesgoJuan Miguel TorralvoPas encore d'évaluation
- Trendelenberg's Test: DR - Ajit DeshmukhDocument16 pagesTrendelenberg's Test: DR - Ajit DeshmukhStar CruisePas encore d'évaluation
- Penile CaDocument76 pagesPenile CaUsmle GuyPas encore d'évaluation
- 2014 Evaluating Anterior Knee PainDocument21 pages2014 Evaluating Anterior Knee PainAni Fran SolarPas encore d'évaluation
- Nejmcp 2032396Document10 pagesNejmcp 2032396juan carlosPas encore d'évaluation
- Dolor Sacro IliacoDocument6 pagesDolor Sacro Iliacomaria antonieta0102Pas encore d'évaluation
- Ankilosig SpondilithisDocument5 pagesAnkilosig SpondilithisFrancois Donatien De SadePas encore d'évaluation
- Kebelet RatnaDocument8 pagesKebelet RatnaOkyWndPas encore d'évaluation
- Blue Book 2011Document222 pagesBlue Book 2011ashokPas encore d'évaluation
- Attending Osteomyelitis ModuleDocument9 pagesAttending Osteomyelitis ModuleMrLarry DolorPas encore d'évaluation
- EpicondilteDocument7 pagesEpicondilteRicardo fariaPas encore d'évaluation
- Persistent Low Back PainDocument8 pagesPersistent Low Back PainAffan MsflPas encore d'évaluation
- Avoiding Common Errors in The Emergency Department-801-1002Document200 pagesAvoiding Common Errors in The Emergency Department-801-1002Hernando CastrillónPas encore d'évaluation
- Lumbarspinalstenosisin Olderadults: Anna M. Lafian,, Karina D. TorralbaDocument12 pagesLumbarspinalstenosisin Olderadults: Anna M. Lafian,, Karina D. TorralbaIhsan KPas encore d'évaluation
- Herniated Nucleus Pulposus TreatmentDocument19 pagesHerniated Nucleus Pulposus Treatmentvicky174Pas encore d'évaluation
- Jake PPDocument31 pagesJake PPapi-323342594Pas encore d'évaluation
- Case Study 3 - Knee PainDocument12 pagesCase Study 3 - Knee PainElizabeth Ho100% (9)
- Acute Back PainDocument6 pagesAcute Back PainWahyudi TriPas encore d'évaluation
- Cervical Spondylosis and Neck PainDocument5 pagesCervical Spondylosis and Neck PainIsaac AlemanPas encore d'évaluation
- Lumbar Radiculopathy Medback Castillo Mendez EDITEDDocument12 pagesLumbar Radiculopathy Medback Castillo Mendez EDITEDSteve ColbertPas encore d'évaluation
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationD'EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehPas encore d'évaluation
- Low Back Pain PDFDocument4 pagesLow Back Pain PDFnetifarhatiiPas encore d'évaluation
- Yulisa 2Document7 pagesYulisa 2Ardi WidiatmikaPas encore d'évaluation
- OU Shoulder and Elbow OITE Review: September 23, 2015 Betsy M. Nolan MDDocument159 pagesOU Shoulder and Elbow OITE Review: September 23, 2015 Betsy M. Nolan MDJayPas encore d'évaluation
- Spondylosis, Degeneration of Intervertebral Disc Diagnosis/Condition: ICD-9 CodesDocument4 pagesSpondylosis, Degeneration of Intervertebral Disc Diagnosis/Condition: ICD-9 CodesAloysius DicodemusPas encore d'évaluation
- Lumbar Disk HerniationDocument6 pagesLumbar Disk HerniationSyarifah Nadya ArfadPas encore d'évaluation
- Cleveland Clinic Journal of Medicine 2007 Klineberg 905 13Document9 pagesCleveland Clinic Journal of Medicine 2007 Klineberg 905 13Sohaib AliPas encore d'évaluation
- Chronic LumbagoDocument8 pagesChronic LumbagoOscar FrizziPas encore d'évaluation
- Clinical Review: Diagnosis and Treatment of Low Back PainDocument5 pagesClinical Review: Diagnosis and Treatment of Low Back PainAulya Adha DiniPas encore d'évaluation
- Jurnal Anastesi 2Document11 pagesJurnal Anastesi 2ainunPas encore d'évaluation
- Hernias AdultosDocument8 pagesHernias AdultosJuan Jose SantivañezPas encore d'évaluation
- Arm 37 717Document4 pagesArm 37 717ChrisPas encore d'évaluation
- Deyo 1992Document6 pagesDeyo 1992Wwwanand111Pas encore d'évaluation
- Lumbar Spine: A Guide For Neurologists Surgical Disorders of The Thoracic andDocument8 pagesLumbar Spine: A Guide For Neurologists Surgical Disorders of The Thoracic andchristian_dyrPas encore d'évaluation
- Spontaneous Regression of A Large Lumbar Disc Extrusion: WWW - Jkns.or - KRDocument3 pagesSpontaneous Regression of A Large Lumbar Disc Extrusion: WWW - Jkns.or - KRAntonius YansenPas encore d'évaluation
- Good Reliability Questionable Validity O20170518 3475 Qhxhhe With Cover Page v2Document183 pagesGood Reliability Questionable Validity O20170518 3475 Qhxhhe With Cover Page v2Ary MfPas encore d'évaluation
- LBP 2Document12 pagesLBP 2Attika DiniPas encore d'évaluation
- Adult Spine 2015Document103 pagesAdult Spine 2015SHARMIN UrmiPas encore d'évaluation
- HNPDocument7 pagesHNPDennyPas encore d'évaluation
- Nonspecific Low Back Pain: Clinical PracticeDocument9 pagesNonspecific Low Back Pain: Clinical PracticeandhikahadiPas encore d'évaluation
- MRI of Degenerative Disease of the Spine: A Case-Based AtlasD'EverandMRI of Degenerative Disease of the Spine: A Case-Based AtlasPas encore d'évaluation
- Exercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509Document4 pagesExercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509herpthederpPas encore d'évaluation
- Nihms452661 PDFDocument11 pagesNihms452661 PDFRaulLopezJaimePas encore d'évaluation
- Handbook of Outpatient MedicineD'EverandHandbook of Outpatient MedicineElana SydneyÉvaluation : 5 sur 5 étoiles5/5 (1)
- March2000 RCP MullerDocument5 pagesMarch2000 RCP MullerMaría José Luengo SepúlvedaPas encore d'évaluation
- Radiculopatia CervicalDocument8 pagesRadiculopatia CervicalFACIVERIPas encore d'évaluation
- Detecting The Differences Radiculopathy, Myelopathy and Peripheral NeuropathyDocument70 pagesDetecting The Differences Radiculopathy, Myelopathy and Peripheral Neuropathyapi-19502000100% (8)
- None 2Document9 pagesNone 2Alfina RahmiPas encore d'évaluation
- Original Paper: Lumbar Disk Herniations - Clinical Status, Diagnosis, Imaging, Surgical Treatment and Global OutcomeDocument6 pagesOriginal Paper: Lumbar Disk Herniations - Clinical Status, Diagnosis, Imaging, Surgical Treatment and Global Outcomeasep budiyantoPas encore d'évaluation
- Jms 21041483Document28 pagesJms 21041483Afra Eslis NoatoPas encore d'évaluation
- Incidental Diagnosis of Intradural Lumbar Disc Herniation During Discography: A Case ReportDocument6 pagesIncidental Diagnosis of Intradural Lumbar Disc Herniation During Discography: A Case ReportVhiena ShittaPas encore d'évaluation
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Document14 pagesNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- Surgical Versus Nonsurgical Therapy For Lumbar Spinal StenosisDocument17 pagesSurgical Versus Nonsurgical Therapy For Lumbar Spinal StenosisAbo ZakariaPas encore d'évaluation
- Lumbar Laminectomy Surgery For Spinal StenosisDocument15 pagesLumbar Laminectomy Surgery For Spinal StenosisElizabeth Liles MartinezPas encore d'évaluation
- ADA 2018 Diabetes CareDocument150 pagesADA 2018 Diabetes CareRoberto López Mata100% (1)
- Best Clinical Practice: AnaphylaxisDocument6 pagesBest Clinical Practice: AnaphylaxisputriPas encore d'évaluation
- Hyperglycemic CrisisDocument9 pagesHyperglycemic CrisisRoberto López MataPas encore d'évaluation
- Fluid Therapy Options and Rational SelectionDocument13 pagesFluid Therapy Options and Rational SelectionRoberto López MataPas encore d'évaluation
- Update On The Management of Venous ThromboembolismDocument8 pagesUpdate On The Management of Venous ThromboembolismRoberto López MataPas encore d'évaluation
- Uric Acid Is A Strong Risk Marker For Developing Hypertension From PrehypertensionDocument16 pagesUric Acid Is A Strong Risk Marker For Developing Hypertension From PrehypertensionRoberto López MataPas encore d'évaluation
- Diagnosis and Treatment of HyperkalemiaDocument9 pagesDiagnosis and Treatment of HyperkalemiaRoberto López MataPas encore d'évaluation
- 2015 ESC Guidelines For The Diagnosis and Management of Pericardial DiseasesDocument44 pages2015 ESC Guidelines For The Diagnosis and Management of Pericardial DiseasesRoberto López MataPas encore d'évaluation
- Pathophysiology of Septic ShockDocument19 pagesPathophysiology of Septic ShockRoberto López MataPas encore d'évaluation
- Rivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeDocument10 pagesRivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeRoberto López MataPas encore d'évaluation
- A Test in Context - D-DimerDocument10 pagesA Test in Context - D-DimerRoberto López MataPas encore d'évaluation
- Diuretic Treatment in Heart FailureDocument12 pagesDiuretic Treatment in Heart FailureRoberto López Mata100% (1)
- Acute Monocular Vision LossDocument9 pagesAcute Monocular Vision LossRoberto López MataPas encore d'évaluation
- Evaluation and Management of Lower-Extremity UlcersDocument9 pagesEvaluation and Management of Lower-Extremity UlcersRoberto López MataPas encore d'évaluation
- Electrolyte Disturbances in Patients With Chronic Alcohol-Use DisorderDocument10 pagesElectrolyte Disturbances in Patients With Chronic Alcohol-Use DisorderRoberto López MataPas encore d'évaluation
- Predicting 30-DayMortality For PatientsWith AcuteHeart Failure in The EmergencyDepartmentDocument14 pagesPredicting 30-DayMortality For PatientsWith AcuteHeart Failure in The EmergencyDepartmentRoberto López MataPas encore d'évaluation
- Indications For and Adverse Effects of Red-Cell TransfusionDocument12 pagesIndications For and Adverse Effects of Red-Cell TransfusionRoberto López Mata100% (1)
- Delirium in Hospitalized Older AdultsDocument11 pagesDelirium in Hospitalized Older AdultsRoberto López MataPas encore d'évaluation
- Will This Hemodynamically Unstable Patient Respond To A Bolus of Intravenous Fluids?Document12 pagesWill This Hemodynamically Unstable Patient Respond To A Bolus of Intravenous Fluids?Roberto López MataPas encore d'évaluation
- Acute Coronary Syndromes The Way Forward From Mechanisms To Precision TreatmentDocument13 pagesAcute Coronary Syndromes The Way Forward From Mechanisms To Precision TreatmentRoberto López MataPas encore d'évaluation
- Social and Psychological Manipulation PDFDocument287 pagesSocial and Psychological Manipulation PDFNicolae BeianPas encore d'évaluation
- Documentary Requirements and Format of Simplified CSHPDocument1 pageDocumentary Requirements and Format of Simplified CSHPRhalf AbnePas encore d'évaluation
- Conization of CervixDocument4 pagesConization of Cervixdrnareshkumar3281Pas encore d'évaluation
- List of Herbal Ingredients Which Are Prohibited or Restricted in MedicinesDocument12 pagesList of Herbal Ingredients Which Are Prohibited or Restricted in MedicinesEtra PublishingPas encore d'évaluation
- Jurnal DysmenorrheaDocument10 pagesJurnal Dysmenorrheaanisah tri agustiniPas encore d'évaluation
- Optimum Detox Foot Pads, Natural Cleansing Ginger Detox Foot PatchesDocument1 pageOptimum Detox Foot Pads, Natural Cleansing Ginger Detox Foot PatchesBrooke GuntherPas encore d'évaluation
- Biology SPMDocument17 pagesBiology SPMbloptra18Pas encore d'évaluation
- Immunity Mark SchemeDocument6 pagesImmunity Mark SchemeDPas encore d'évaluation
- Invuity Investor Presentation - Q3 2017Document22 pagesInvuity Investor Presentation - Q3 2017medtechyPas encore d'évaluation
- DRISHTIDocument1 pageDRISHTIsumitha SPas encore d'évaluation
- TLIC107C - Drive Vehicle - Learner GuideDocument101 pagesTLIC107C - Drive Vehicle - Learner GuideromerofredPas encore d'évaluation
- Ge Cumulative Rates ResortedDocument81 pagesGe Cumulative Rates ResortedfishyfredPas encore d'évaluation
- FP TrainedProviders 2Document9 pagesFP TrainedProviders 2Bharma LogisticsPas encore d'évaluation
- PIL 18047 LatestDocument2 pagesPIL 18047 LatestWendy EscalantePas encore d'évaluation
- History Taking and MSE AIIMS PatnaDocument34 pagesHistory Taking and MSE AIIMS PatnaShivendra Kumar100% (1)
- Biopotential Amplifiers 2Document52 pagesBiopotential Amplifiers 2Jesus Peña100% (1)
- Connectors in FPDDocument53 pagesConnectors in FPDsrinivaskalluri80% (5)
- TRMDLDocument5 pagesTRMDLrizkaPas encore d'évaluation
- Unite - October 2013Document40 pagesUnite - October 2013Bruce SeamanPas encore d'évaluation
- Radiopharmaceuticals & Nuclear PharmacyDocument39 pagesRadiopharmaceuticals & Nuclear PharmacyKhalid HussainPas encore d'évaluation
- Clinic: Klinikos Is Sloping or Reclining and Latin Is ClinicusDocument3 pagesClinic: Klinikos Is Sloping or Reclining and Latin Is Clinicusfl004Pas encore d'évaluation
- Nabh Entry LevelDocument64 pagesNabh Entry LevelRenuka MuruganPas encore d'évaluation
- Conservative Treatment, Plate Fixation, or Prosthesis For Proximal Humeral Fracture. A Prospective Randomized StudyDocument3 pagesConservative Treatment, Plate Fixation, or Prosthesis For Proximal Humeral Fracture. A Prospective Randomized StudyAndi Urviana AsrahPas encore d'évaluation
- Erotic HypnosisDocument148 pagesErotic HypnosisNeha93% (27)
- German Marine Agencies, Inc., Et Al. Petitioners, vs. Teodolah R. Caro, in Behalf of Her Husband Eduardo v. Caro, Respondent.Document5 pagesGerman Marine Agencies, Inc., Et Al. Petitioners, vs. Teodolah R. Caro, in Behalf of Her Husband Eduardo v. Caro, Respondent.Francis Coronel Jr.Pas encore d'évaluation
- Sound TherapyDocument1 pageSound TherapyibedaflyPas encore d'évaluation
- Radial Head FractureDocument40 pagesRadial Head FractureammarPas encore d'évaluation
- At The PharmacyDocument6 pagesAt The PharmacyCristian González GonzálezPas encore d'évaluation
- Republic Act MnemonicsDocument3 pagesRepublic Act MnemonicsJill P100% (1)
- Frog Dissection LabDocument6 pagesFrog Dissection Labapi-279500653Pas encore d'évaluation