Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Effect of Lower Extremity Muscular Fatigue On Motor Control PerformanceDocument21 pagesEffect of Lower Extremity Muscular Fatigue On Motor Control PerformancePabloT81Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- An Anatomic Investigation of The Ober TestDocument7 pagesAn Anatomic Investigation of The Ober TestPabloT81Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Velocity-Based Training in FootballDocument7 pagesVelocity-Based Training in FootballPabloT81Pas encore d'évaluation
- In-Season Weightlifting Training Exercise in Healthy Male Handball Players: E Muscle Volume, Maximal Strength, and Ball-Throwing VelocityDocument14 pagesIn-Season Weightlifting Training Exercise in Healthy Male Handball Players: E Muscle Volume, Maximal Strength, and Ball-Throwing VelocityPabloT81Pas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Practical Applications of Biomechanical Principles in Resistance TrainingDocument17 pagesPractical Applications of Biomechanical Principles in Resistance TrainingPabloT81Pas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Long Distance Running and Knee Osteoarthritis A Prospective StudyDocument10 pagesLong Distance Running and Knee Osteoarthritis A Prospective StudyPabloT81Pas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Analysis of Scapular Muscle EMG Activity in Patients With Idiopathic Neck Pain. A Systematic ReviewDocument16 pagesAnalysis of Scapular Muscle EMG Activity in Patients With Idiopathic Neck Pain. A Systematic ReviewPabloT81Pas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Motion Analysis of U11 To U16 Elite English PremierDocument12 pagesMotion Analysis of U11 To U16 Elite English PremierPabloT81Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- CS3501 Compiler Design Lab ManualDocument43 pagesCS3501 Compiler Design Lab ManualMANIMEKALAIPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Green ThumbDocument2 pagesGreen ThumbScarlet Sofia Colmenares VargasPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
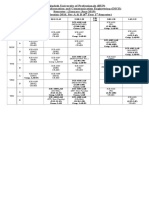
- Class Routine Final 13.12.18Document7 pagesClass Routine Final 13.12.18RakibPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Aristotle Metaphysics Lambda Accessed 201111 Classicalk LibraryDocument19 pagesAristotle Metaphysics Lambda Accessed 201111 Classicalk Librarygijsbo2000Pas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Schmidt Hammer TestDocument5 pagesSchmidt Hammer Testchrtrom100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- SoundsDocument61 pagesSoundsJemabel RosarioPas encore d'évaluation
- LQZLQM ) So"L/L6H Klans LN : Sfof (No K - Of) HGSF) Nflu DFQDocument5 pagesLQZLQM ) So"L/L6H Klans LN : Sfof (No K - Of) HGSF) Nflu DFQSAJAL KOIRALAPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Bosch KE-Jetronic System DescriptionDocument3 pagesBosch KE-Jetronic System DescriptionJack Tang50% (2)
- Flow Through A Converging-Diverging Tube and Its Implications in Occlusive Vascular Disease-IDocument9 pagesFlow Through A Converging-Diverging Tube and Its Implications in Occlusive Vascular Disease-IRukhsarAhmedPas encore d'évaluation
- Managing Markets Strategically: Professor Noel CaponDocument49 pagesManaging Markets Strategically: Professor Noel CaponChristiandeuxPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Electronic Parts Catalog - Option Detail Option Group Graphic Film Card DateDocument2 pagesElectronic Parts Catalog - Option Detail Option Group Graphic Film Card DatenurdinzaiPas encore d'évaluation
- Emcee Script For Recognition DayDocument3 pagesEmcee Script For Recognition DayRomeo Jr. LaguardiaPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- ANNEXESDocument6 pagesANNEXESKyzer Calix LaguitPas encore d'évaluation
- 1st Unseen Passage For Class 5 in EnglishDocument7 pages1st Unseen Passage For Class 5 in EnglishVibhav SinghPas encore d'évaluation
- Problems: C D y XDocument7 pagesProblems: C D y XBanana QPas encore d'évaluation
- Effect of Minor and Trace Elements in Cast IronDocument2 pagesEffect of Minor and Trace Elements in Cast IronsachinguptachdPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Contribution of Medieval MuslimDocument16 pagesContribution of Medieval Muslimannur osmanPas encore d'évaluation
- Bilateral Transfer of LearningDocument18 pagesBilateral Transfer of Learningts2200419Pas encore d'évaluation
- تأثير العناصر الثقافية والبراغماتية الأسلوبية في ترجمة سورة الناس من القرآن الكريم إلى اللغة الإ PDFDocument36 pagesتأثير العناصر الثقافية والبراغماتية الأسلوبية في ترجمة سورة الناس من القرآن الكريم إلى اللغة الإ PDFSofiane DouifiPas encore d'évaluation
- Hume 100 ReviewerDocument7 pagesHume 100 ReviewerShai GaviñoPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Bamboo People - An Interdisciplinary Unit For High SchoolDocument6 pagesBamboo People - An Interdisciplinary Unit For High SchoolChipo Jean MarundaPas encore d'évaluation
- EEE301 Digital Electronics Lecture 1 Part 3: Dr. A.S.M. MohsinDocument6 pagesEEE301 Digital Electronics Lecture 1 Part 3: Dr. A.S.M. MohsinAaa AaaPas encore d'évaluation
- TransistorDocument3 pagesTransistorAndres Vejar Cerda0% (1)
- Lesson Exemplar Math 7Document6 pagesLesson Exemplar Math 7Pablo Jimenea100% (2)
- College of Engineering Cagayan State UniversityDocument16 pagesCollege of Engineering Cagayan State UniversityErika Antonio GutierrezPas encore d'évaluation
- NiftDocument3 pagesNiftMegha Nair PillaiPas encore d'évaluation
- Scan WV1DB12H4B8018760 20210927 1800Document6 pagesScan WV1DB12H4B8018760 20210927 1800Sergio AlvarezPas encore d'évaluation
- T54125ADocument64 pagesT54125ARaúl FroddenPas encore d'évaluation
- Shift Registers NotesDocument146 pagesShift Registers NotesRajat KumarPas encore d'évaluation
- Manitou 1350RDocument4 pagesManitou 1350RcandlaganPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)