Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Association Between MRNA Expression of Aromatase 1Document8 pagesAssociation Between MRNA Expression of Aromatase 1Nenny Yoanitha DjalaPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Palliative Care - Modul NennyDocument31 pagesPalliative Care - Modul NennyNenny Yoanitha DjalaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
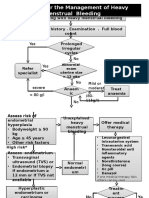
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- American Journal of Obstetrics and Gynecology Volume 207 Issue 3 2012 (Doi 10.1016/j.ajog.2012.07.031) McPherson, Jessica A. Odibo, Anthony O. Shanks, Anthony L. Ro - Impact of Chorionicity On R PDFDocument6 pagesAmerican Journal of Obstetrics and Gynecology Volume 207 Issue 3 2012 (Doi 10.1016/j.ajog.2012.07.031) McPherson, Jessica A. Odibo, Anthony O. Shanks, Anthony L. Ro - Impact of Chorionicity On R PDFNenny Yoanitha DjalaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Night Shift Duty 11 FEBRUARIDocument2 pagesNight Shift Duty 11 FEBRUARINenny Yoanitha DjalaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Hypertensionin PregnancyDocument100 pagesHypertensionin Pregnancyricky hutagalungPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Program Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Document1 pageProgram Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Nenny Yoanitha DjalaPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Estimated Fetal Weight Formula GuideDocument5 pagesEstimated Fetal Weight Formula GuideNenny Yoanitha Djala100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaPas encore d'évaluation
- En Endometrial Cancer Guide For PatientsDocument30 pagesEn Endometrial Cancer Guide For PatientsNenny Yoanitha DjalaPas encore d'évaluation
- AJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenDocument6 pagesAJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenNenny Yoanitha DjalaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Medical Eligibility Criteria For Contraceptive Use Fifth Edition 2015Document14 pagesMedical Eligibility Criteria For Contraceptive Use Fifth Edition 2015agustinasntPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Termination Pregnancy Report 18 May 2010Document45 pagesTermination Pregnancy Report 18 May 2010Nenny Yoanitha DjalaPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Final Data 2011 PDFDocument90 pagesFinal Data 2011 PDFNenny Yoanitha DjalaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Anatomical Causes Bad Obstetric HistoryDocument3 pagesAnatomical Causes Bad Obstetric Historykyle31Pas encore d'évaluation
- Strategi Bisnis KorporasiDocument41 pagesStrategi Bisnis KorporasiAliMu'minHarahapPas encore d'évaluation
- Forceps Review in Modern Obstetric PracticeDocument5 pagesForceps Review in Modern Obstetric PracticeNenny Yoanitha DjalaPas encore d'évaluation
- Fetal and Maternal Effects of Forceps and VacuumDocument4 pagesFetal and Maternal Effects of Forceps and VacuumNenny Yoanitha DjalaPas encore d'évaluation
- How To Explore After Forceps ExtractionDocument7 pagesHow To Explore After Forceps ExtractionNenny Yoanitha DjalaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaPas encore d'évaluation
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaPas encore d'évaluation
- Trali Dari Ats JournalDocument2 pagesTrali Dari Ats JournalNenny Yoanitha DjalaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Successful Pregnancy OutcomeDocument6 pagesSuccessful Pregnancy OutcomeNenny Yoanitha DjalaPas encore d'évaluation
- Forceps ExtractionDocument49 pagesForceps ExtractionNenny Yoanitha DjalaPas encore d'évaluation
- Obstetrical Forceps - History Mystery and MoralityDocument16 pagesObstetrical Forceps - History Mystery and MoralityNenny Yoanitha DjalaPas encore d'évaluation
- Cytomegalovirus Infection in Patients With Active InflammatoryDocument7 pagesCytomegalovirus Infection in Patients With Active InflammatoryNenny Yoanitha DjalaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Genetic Study of TORCH Infections in Women With BOH PDFDocument6 pagesGenetic Study of TORCH Infections in Women With BOH PDFNenny Yoanitha DjalaPas encore d'évaluation
- Pregnancy Induced HypertentionDocument2 pagesPregnancy Induced Hypertentionapi-31064465050% (2)
- Initiation and Maintenance of Labour Analgesia: Epidural or CSE, Bolus or InfusionDocument32 pagesInitiation and Maintenance of Labour Analgesia: Epidural or CSE, Bolus or Infusionleo chiuPas encore d'évaluation
- ATI Maternal Newborn Chapter 1-ContraceptionDocument23 pagesATI Maternal Newborn Chapter 1-ContraceptionVin Lorenzo Campbell100% (4)
- Pregnancy Stages GuideDocument15 pagesPregnancy Stages Guidefarhan_ansPas encore d'évaluation
- 2nd Stage of LabourDocument153 pages2nd Stage of LabourBhawna Joshi100% (1)
- SEO-Optimized Title for Document on Various Gynecological and Obstetric TopicsDocument140 pagesSEO-Optimized Title for Document on Various Gynecological and Obstetric TopicsjPas encore d'évaluation
- Cruzada, Marjorie J. NCM 107-Care of Mother, Child and Adolescent Define or Give Brief Description For Each of The Obstetric TermsDocument6 pagesCruzada, Marjorie J. NCM 107-Care of Mother, Child and Adolescent Define or Give Brief Description For Each of The Obstetric TermsRea Jane Astrologo PastorPas encore d'évaluation
- Term Paper 2nd YearDocument83 pagesTerm Paper 2nd YearJomy Suneesh100% (1)
- NCM 107 Skills Lab NCPDocument1 pageNCM 107 Skills Lab NCPMoises Clerick BalloguingPas encore d'évaluation
- Mark Klimek NotesDocument25 pagesMark Klimek NotesJenina OPas encore d'évaluation
- Obstetrics Nursing Questions Answer KeyDocument13 pagesObstetrics Nursing Questions Answer Keyicy431100% (2)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Jurnal Aroma TerapiDocument246 pagesJurnal Aroma Terapidewi100% (1)
- A. 1. Nursing Care of The High Risk Newborn To MaturityDocument30 pagesA. 1. Nursing Care of The High Risk Newborn To MaturityRika MaePas encore d'évaluation
- Form F Registration RecordDocument2 pagesForm F Registration RecordArchit ChampanekarPas encore d'évaluation
- Developing SMART Objectives Case StudyDocument3 pagesDeveloping SMART Objectives Case StudyVarun AchrejaPas encore d'évaluation
- Lebanon - Congenital Anomalies Prevalence and Risk FactorsDocument7 pagesLebanon - Congenital Anomalies Prevalence and Risk FactorsAbdelrhman WagdyPas encore d'évaluation
- IWKDocument5 pagesIWKjclavel4314Pas encore d'évaluation
- Expanded Maternity Leave LawDocument58 pagesExpanded Maternity Leave LawAnalyn Grace BasayPas encore d'évaluation
- FULL Guideline SOGC 2005 2016Document756 pagesFULL Guideline SOGC 2005 2016dr.razi100% (1)
- Measuring fertility and mortality ratesDocument3 pagesMeasuring fertility and mortality ratesAnis Elina ZulkipliPas encore d'évaluation
- Umbilical cord prolapse emergencyDocument19 pagesUmbilical cord prolapse emergencydenekePas encore d'évaluation
- Abnormal LaborDocument84 pagesAbnormal LaborMi MaymdPas encore d'évaluation
- Đề Thi Khảo Sát Chất Lượng Môn Tiếng AnhDocument50 pagesĐề Thi Khảo Sát Chất Lượng Môn Tiếng AnhVân Minh ThiPas encore d'évaluation
- Nursing BulletsDocument83 pagesNursing BulletsgilissaPas encore d'évaluation
- Case Study - Full-Term BabyDocument32 pagesCase Study - Full-Term BabyMarron Jane GanoticePas encore d'évaluation
- Labor and DeliveryDocument70 pagesLabor and DeliveryャチPas encore d'évaluation
- DocxDocument12 pagesDocxJojo JacobPas encore d'évaluation
- Ventouse ExtractionDocument3 pagesVentouse ExtractionNishaThakuriPas encore d'évaluation
- Hospital Department DefinitionsDocument9 pagesHospital Department DefinitionsHanafi S KepPas encore d'évaluation
- NCM 109 ReviewerDocument8 pagesNCM 109 ReviewerAlma Janella TOSINO100% (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (402)