Vous aimerez peut-être aussi
- Siddharth Agrawal - Strabismus - For Every Ophthalmologist-Springer Singapore (2019) PDFDocument177 pagesSiddharth Agrawal - Strabismus - For Every Ophthalmologist-Springer Singapore (2019) PDFMischell Lázaro Ordonio100% (1)
- MicroPulse - P3 Rev 2 - Cyan MedicaDocument6 pagesMicroPulse - P3 Rev 2 - Cyan MedicaMischell Lázaro OrdonioPas encore d'évaluation
- Etiology and evaluation of hematuria in adultsDocument16 pagesEtiology and evaluation of hematuria in adultsMischell Lázaro OrdonioPas encore d'évaluation
- Secondary Prevention Early Onset GBS Disease Among NewbornsDocument1 pageSecondary Prevention Early Onset GBS Disease Among NewbornsMischell Lázaro OrdonioPas encore d'évaluation
- Systemic Effects of Perinatal AsphyxiaDocument7 pagesSystemic Effects of Perinatal AsphyxiaMischell Lázaro OrdonioPas encore d'évaluation
- Hematuria ClasificacionDocument4 pagesHematuria ClasificacionMischell Lázaro OrdonioPas encore d'évaluation
- Current Concepts in The Pathogenesis andDocument14 pagesCurrent Concepts in The Pathogenesis andMischell Lázaro OrdonioPas encore d'évaluation
- Findings Neonatal SepsisDocument1 pageFindings Neonatal SepsisMischell Lázaro OrdonioPas encore d'évaluation
- Clinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm InfantsDocument12 pagesClinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm InfantsMischell Lázaro OrdonioPas encore d'évaluation
- Bacteria Sepsis Term InfantDocument1 pageBacteria Sepsis Term InfantMischell Lázaro OrdonioPas encore d'évaluation
- Neonatal Sepsis Differential DiagnosisDocument1 pageNeonatal Sepsis Differential DiagnosisMischell Lázaro OrdonioPas encore d'évaluation
- Docena DiabetesDocument3 pagesDocena DiabetesMischell Lázaro OrdonioPas encore d'évaluation
- Pancreatitis 2015Document35 pagesPancreatitis 2015Mischell Lázaro OrdonioPas encore d'évaluation
- Chep 2016Document70 pagesChep 2016Mischell Lázaro OrdonioPas encore d'évaluation
- 1 Octeto de DefronzoDocument23 pages1 Octeto de DefronzoLesli Rodriguez50% (2)
- Hematuria ClasificacionDocument4 pagesHematuria ClasificacionMischell Lázaro OrdonioPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Paraphimosis (Ingles)Document1 pageParaphimosis (Ingles)Joaquín SosaPas encore d'évaluation
- Interstitial Cystitis (Bladder Inflammation) - ColumbiaDoctors - New YorkDocument6 pagesInterstitial Cystitis (Bladder Inflammation) - ColumbiaDoctors - New YorkJimmy GillPas encore d'évaluation
- SOP: Urinary Catheter in Dogs and CatsDocument6 pagesSOP: Urinary Catheter in Dogs and CatsMas HendryPas encore d'évaluation
- The TURP Procedure StepDocument3 pagesThe TURP Procedure Stepnorhafizahstoh89100% (1)
- Confirmed COVID-19 Confirmed COVID-19Document5 pagesConfirmed COVID-19 Confirmed COVID-19ilham masdarPas encore d'évaluation
- Effects of Transurethral Resection of Prostate (Turp) On Uroflowmetry Parameters On Patients Having Benign Prostatic HyperplasiaDocument6 pagesEffects of Transurethral Resection of Prostate (Turp) On Uroflowmetry Parameters On Patients Having Benign Prostatic HyperplasiaKamran AfzalPas encore d'évaluation
- Urinary Infections in The ElderlyDocument29 pagesUrinary Infections in The ElderlyChris FrenchPas encore d'évaluation
- Quick Start Guides For Urodynamics Testing V06 (MAN247)Document62 pagesQuick Start Guides For Urodynamics Testing V06 (MAN247)prathibhasaseedharanPas encore d'évaluation
- Management of Renal Stones: Theme From January 2013 ExamDocument123 pagesManagement of Renal Stones: Theme From January 2013 ExamBela VitoriaPas encore d'évaluation
- 4 - Surgical Treatment of BPHDocument55 pages4 - Surgical Treatment of BPHKsatria DressrosaPas encore d'évaluation
- CGHS Chennai Empanelled Hospital List As On Apr 23Document7 pagesCGHS Chennai Empanelled Hospital List As On Apr 23Banumathy RajappaPas encore d'évaluation
- UrethralbladderinjuryDocument32 pagesUrethralbladderinjuryNinaPas encore d'évaluation
- Pelvic Inflammatory DiseaseDocument4 pagesPelvic Inflammatory DiseasekabebangPas encore d'évaluation
- Ureteroscopy Techniques and Outcomes for Treating Kidney Stones and CancerDocument66 pagesUreteroscopy Techniques and Outcomes for Treating Kidney Stones and CancerCentanarianPas encore d'évaluation
- Catheterization ProcedureDocument3 pagesCatheterization ProcedureAbigail BascoPas encore d'évaluation
- Genitourinary trauma guideDocument42 pagesGenitourinary trauma guideOrin SujasmanPas encore d'évaluation
- Sales & Distribution Project: Contraceptive Condom DurexDocument32 pagesSales & Distribution Project: Contraceptive Condom DurexManish NeerajPas encore d'évaluation
- Referensiii NefrotiasisDocument6 pagesReferensiii NefrotiasisPramestiPas encore d'évaluation
- Case-Urinary Catheterizarion DR - PNTDocument38 pagesCase-Urinary Catheterizarion DR - PNTWan Adi OeyaPas encore d'évaluation
- FELINE URETERAL OBSTRUCTION MANAGEMENTDocument6 pagesFELINE URETERAL OBSTRUCTION MANAGEMENTvetgaPas encore d'évaluation
- Morcellation From KARL STORZDocument20 pagesMorcellation From KARL STORZimbesil123Pas encore d'évaluation
- Bagian Kedua Tes Bahasa Inggris (Nomor 121 S.D. 180) Structure and Written ExpressionDocument5 pagesBagian Kedua Tes Bahasa Inggris (Nomor 121 S.D. 180) Structure and Written ExpressionFredy Allan SusantoPas encore d'évaluation
- Indwelling Urinary CatheterizationDocument8 pagesIndwelling Urinary CatheterizationNiña Jean Tormis AldabaPas encore d'évaluation
- Treatmen UrologiDocument681 pagesTreatmen UrologisulthonPas encore d'évaluation
- Urinary Tract Infection - FinalDocument86 pagesUrinary Tract Infection - FinalShreyance Parakh100% (1)
- Tractus Urinarius: Departemen Anatomi Fk-Usu MedanDocument21 pagesTractus Urinarius: Departemen Anatomi Fk-Usu MedanRizky Indah SorayaPas encore d'évaluation
- 4 - CatheterizationDocument20 pages4 - Catheterizationkirstenfrancine28Pas encore d'évaluation
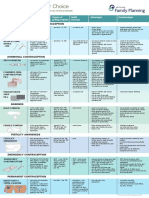
- Contraception Options in New ZealandDocument2 pagesContraception Options in New ZealandStuff NewsroomPas encore d'évaluation
- UroLap 2.0 - BrochureDocument3 pagesUroLap 2.0 - Brochurehindi channelPas encore d'évaluation
- Urinary RetentionDocument28 pagesUrinary RetentionSchoeb MuhammadPas encore d'évaluation