Vous aimerez peut-être aussi
- ARIA Report 2008Document196 pagesARIA Report 2008jasbroPas encore d'évaluation
- Ondansentron in Diarrhea PDFDocument8 pagesOndansentron in Diarrhea PDFPhilipus Putra RaharjoPas encore d'évaluation
- Renal TraumaDocument53 pagesRenal TraumaPhilipus Putra RaharjoPas encore d'évaluation
- Acute Kidney Injury - Final Version (08 March 2011)Document59 pagesAcute Kidney Injury - Final Version (08 March 2011)Abdel-hafiz MamounPas encore d'évaluation
- Mcgraw-Hill: Deep Pain From Visceral and Skeletomuscular Structures IsDocument2 pagesMcgraw-Hill: Deep Pain From Visceral and Skeletomuscular Structures IsPhilipus Putra RaharjoPas encore d'évaluation
- Acute Kidney Injury (QS76) - ClinicalKeyDocument28 pagesAcute Kidney Injury (QS76) - ClinicalKeyPhilipus Putra RaharjoPas encore d'évaluation
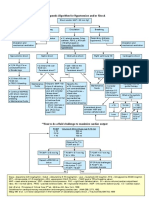
- Therapeutic Algorithm For HypotensionDocument1 pageTherapeutic Algorithm For HypotensionPhilipus Putra RaharjoPas encore d'évaluation
- Moles and Skin LesionsDocument5 pagesMoles and Skin LesionsPhilipus Putra RaharjoPas encore d'évaluation
- Absorbed Into The Blood From Its Site of Administration and Distributed To Its Site of ActionDocument9 pagesAbsorbed Into The Blood From Its Site of Administration and Distributed To Its Site of ActionPhilipus Putra RaharjoPas encore d'évaluation
- Propionic AcidemiaDocument4 pagesPropionic AcidemiaPhilipus Putra RaharjoPas encore d'évaluation
- There Are Two Types of Nociceptors Corresponding ToDocument6 pagesThere Are Two Types of Nociceptors Corresponding ToPhilipus Putra RaharjoPas encore d'évaluation
- Digital MedicineDocument223 pagesDigital MedicinePhilipus Putra RaharjoPas encore d'évaluation
- Jet LagDocument7 pagesJet LagPhilipus Putra RaharjoPas encore d'évaluation
- McKinley Health CenterDocument4 pagesMcKinley Health CenterPhilipus Putra RaharjoPas encore d'évaluation
- The Primary Survey: Cervical Spine Management Chapter 1.12Document5 pagesThe Primary Survey: Cervical Spine Management Chapter 1.12Philipus Putra RaharjoPas encore d'évaluation
- Leukemia - Topic OverviewDocument5 pagesLeukemia - Topic OverviewPhilipus Putra RaharjoPas encore d'évaluation
- At A Glace MedicineDocument365 pagesAt A Glace MedicinePhilipus Putra RaharjoPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Quiz 7. NCM 116 For StudentsDocument4 pagesQuiz 7. NCM 116 For StudentsZayne Lucas Gabrielle TadiamonPas encore d'évaluation
- Covid 19 Infographic enDocument1 pageCovid 19 Infographic enTrilok AshpalPas encore d'évaluation
- Test CaeDocument3 pagesTest CaegabiPas encore d'évaluation
- Vinyl Chloride MonomerDocument6 pagesVinyl Chloride MonomerRizqia Putri ZakkaPas encore d'évaluation
- Research On DOH Approved Herbal MedicinesDocument31 pagesResearch On DOH Approved Herbal Medicinesfilithesis79% (14)
- Nursing Health Assessment Guide: San Pedro CollegeDocument3 pagesNursing Health Assessment Guide: San Pedro CollegeRue Cheng MaPas encore d'évaluation
- Page From Thompson Thompson Genetics in Medicine 8Document2 pagesPage From Thompson Thompson Genetics in Medicine 8jorgegrodlPas encore d'évaluation
- Structural Organisation in AnimalsDocument23 pagesStructural Organisation in AnimalsMothi KarunaPas encore d'évaluation
- FIN255 Answer Key 4Document4 pagesFIN255 Answer Key 4Wendz RepaldaPas encore d'évaluation
- CeftriaxoneDocument7 pagesCeftriaxoneGreats HalomoanPas encore d'évaluation
- Germ Theory of Diseases Von PlencizDocument2 pagesGerm Theory of Diseases Von PlencizAamni SinghPas encore d'évaluation
- Corporate Yoga & Stress ArticlesDocument11 pagesCorporate Yoga & Stress Articless.gnanasekaranPas encore d'évaluation
- AHA18HyperPocketGuidePRINT3FINAL APPROVED PDFDocument2 pagesAHA18HyperPocketGuidePRINT3FINAL APPROVED PDFAmanda JulianaPas encore d'évaluation
- Veterinary OniometerDocument2 pagesVeterinary OniometerAmarnath MuthukrishnanPas encore d'évaluation
- Culture and ObesityDocument6 pagesCulture and ObesityShabi ZeePas encore d'évaluation
- Group WorkDocument19 pagesGroup WorkSoumya Ranjan ParidaPas encore d'évaluation
- Classroom Activity HLTWHS002Document6 pagesClassroom Activity HLTWHS002Sonam Gurung100% (1)
- Infectious Diseases and Their Treatment in Georgian Written SourcesDocument21 pagesInfectious Diseases and Their Treatment in Georgian Written SourcesIrina GogonaiaPas encore d'évaluation
- Scott Foresman Science Grade 4Document8 pagesScott Foresman Science Grade 4rofi modiPas encore d'évaluation
- Gicaro CED101IEWrittenOutputDocument15 pagesGicaro CED101IEWrittenOutputAlyssa GicaroPas encore d'évaluation
- 3 Biological Macromolecules: Chapter OutlineDocument35 pages3 Biological Macromolecules: Chapter OutlineMarkus EvanPas encore d'évaluation
- Equine Field SurgeryDocument6 pagesEquine Field SurgeryRuchiPas encore d'évaluation
- Pathology Lec 1Document16 pagesPathology Lec 1hamadPas encore d'évaluation
- Asbestos Awareness Quiz #1: AnswersDocument2 pagesAsbestos Awareness Quiz #1: AnswersMichael NcubePas encore d'évaluation
- Endocrine SystemDocument4 pagesEndocrine SystemCELLINA CLARISSE DE LEONPas encore d'évaluation
- Common Types of StrabismusDocument9 pagesCommon Types of Strabismustasya noerchaerunisaPas encore d'évaluation
- Scabies NotesDocument9 pagesScabies NotesAvi ePas encore d'évaluation
- Left Atrial Function: Physiology, Assessment, and Clinical ImplicationsDocument10 pagesLeft Atrial Function: Physiology, Assessment, and Clinical ImplicationsfitriasyrofianaPas encore d'évaluation
- Pschology 2Document35 pagesPschology 2Sarah Mae SaringanPas encore d'évaluation
- AAOS 2018 Foot and Ankle - by KhawajaDocument108 pagesAAOS 2018 Foot and Ankle - by KhawajaChristopherLawrencePas encore d'évaluation